One of this article’s authors, Omar A. Barrada, MD, was a witness to the violence associated with the 2011 January 25th Revolution in Egypt. At the time, Dr. Barrada was completing his vitreoretinal fellowship at El Kasr El Aini, Cairo University’s 100-year-old teaching hospital and by far Egypt’s biggest referral center.
Dr. Barrada was awarded honorary certificates by Cairo University Medical School and The Egyptian Doctor’s Syndicate for his efforts in treating the wounded during the January 25th Revolution.
The period called the Arab Spring occurred between January 2011 and January 2013. During these 2 years multiple revolutions sprang up across the Middle East and Northern Africa. Repeated standoffs between security forces and the general public and between different factions of the populations of these countries took place. A few people lost their lives, and a lot of people lost their eyes. The low-caliber gunshot was the weapon of choice for the security forces, used to disperse the masses, as well as for the population in resolving unfriendly skirmishes in some of Egypt’s dodgiest neighborhoods.
Gunshot injuries to the face can present to the ophthalmologist in a number of ways. According to the Birmingham Eye Trauma Terminology System (BETTS), gunshot injuries to the eye are usually of the open-globe variety, and rarely of the closed-globe variety.1 Of the open-globe variety, the most commonly encountered clinical presentations are penetrating injuries, characterized by an entrance wound and intraocular foreign body (IOFB), or perforating injuries characterized by both an entrance and an exit wound with the foreign body impacted in the orbital tissue behind the eye.

Figure 1. A corneal entry wound.

Figure 2. A scleral entry wound.

Figure 3. X-ray shows multiple metallic pellets in the head and neck; notice the multiple foreign bodies in the orbital cavity.

Figure 4. Severe corneal edema and hyphema. Vitrectomy with visualization through such a cornea is impossible.

Figure 5. Dense, organized, layered vitreous hemorrhage.
When an ophthalmologist encounters such cases, he or she should have a short checklist to go through, which should include the following:
- Are there concurrent systemic injuries that necessitate the consultation of a specialist; ie, is the patient’s life in danger due to his injuries?
- Complete and thorough history should be taken, concentrating on the circumstances in which the patient sustained his or her injuries (for medicolegal issues).
- Visual acuity should be carefully tested and documented.
- The anterior segment should be examined with meticulous care directed to identifying the entrance wound (Figures 1 and 2); note that there may be more than 1 IOFB, and therefore more than 1 entrance wound.
- Posterior segment examination is usually not possible, as these injuries are usually associated with dense media opacities that do not allow direct visualization of the retina.
- Imaging investigations should be conducted; x-ray (Figure 3) and computed tomography scan of the brain and orbits are the imaging modalities of choice. Magnetic resonance imaging is contraindicated in gunshot injuries, as it can cause a metallic IOFB to move, thus causing greater injury to the eye. Ultrasound B-scan should be delayed until primary closure of all wounds is achieved.
PRIMARY INTERVENTION
How to initially proceed in eyes with gunshot injuries is debatable. In all cases, prompt and meticulous closure of all entrance wounds is of utmost importance. Then, depending on the type of injury, further interventions can be considered. If the injury is of the perforating type, with both an entrance and an exit wound, primary vitrectomy is not advised, as the posteriorly located exit wound will allow the fluid infused into the eye to egress, and collapse of the globe during surgery is likely.
If the injury is of the penetrating type with an IOFB, the first surgical decision must be made: Should you proceed with a vitrectomy and remove the IOFB in the primary procedure, or should you be satisfied with primary closure of the wound and schedule the vitrectomy for a later date? The answer depends on the clarity of the cornea. If the cornea is the site of pellet entry, or if it is too edematous, hampering visualization, then vitrectomy will be impossible and should be postponed (Figure 4).
SECONDARY INTERVENTION
The ideal timing to perform a secondary vitrectomy is unknown. Variables that influence the decision of when to intervene include spontaneous, watertight healing and closure of the exit wound and the restoration of corneal transparency.
Provided that a narrow window of clear cornea is available, advances in wide-angle viewing systems, such as the Binocular Indirect Ophthalmomicroscope (BIOM; Oculus), allow surgery to be performed through a markedly opaque cornea. If that window into the eye is not present, then vitrectomy through a temporary keratoprosthesis is the surgeon’s only option. Waiting for 1 to 3 weeks before proceeding with the secondary intervention is advisable to allow enough time to pass for the exit wound to heal and for posterior vitreous detachment (PVD) to occur, making surgery safer and much easier to perform.

Figure 6. The metallic IOFB was removed through an enlarged 20-gauge sclerotomy.
SURGICAL TECHNIQUE
Vitrectomy for gunshot injuries varies greatly from case to case, and each should be tackled in a tailored manner. When preparing for surgery the surgeon must consider several points:
- Will the cornea allow adequate visualization of the posterior segment?
- Is there an associated cataract?
- Is the retina detached?
- Is there an IOFB?
- What size instruments should be used?
If the cornea is too opaque or damaged, a temporary keratoprosthesis can be used and a donor cornea sutured in place after the completion of the vitrectomy. If there is an associated cataract, it must be removed in order to adequately visualize the posterior segment. The question of whether an intraocular lens (IOL) should be implanted at the same surgical session is debatable. If the retina is detached, the best choice is not to implant an IOL but to save that step for a later date. If the patient is young and the crystalline lens soft, a pars plana lensectomy with polishing but preservation of the anterior capsule can be performed. The patient should be followed until his or her retinal condition is stable, and then a secondary sulcus IOL implantation can be planned.
Because of the very dense, organized vitreous hemorrhage associated with such trauma, clear differentiation between tissues can be difficult (Figure 5). While removing the layers of hemorrhage, the surgeon must be very careful not to injure the underlying retina. One trick is to try to create a small hole into the organized fibrous tissue and sneak a peek into it in order to assess the retinal status.

Figure 7. Postoperative diffuse epiretinal fibrosis.

Figure 8. Silicone-filled vitreous cavity with severe fibrosis at the site of the exit wound.
If the injury is of the perforating type, the track formed by the pellet as it moves through the eye organizes and becomes fibrosed. The exit wound is usually surrounded by an amalgam of vitreous, blood, and ocular tissue, which acts as a plug, sealing that wound. When these plugs are removed, close but not complete shaving is sufficient, and usually the application of laser barrage around it is unnecessary.
REMOVAL OF IOFBs
After the hemorrhage is cleared, the next step is the removal of the IOFB, if present. IOFBs should always be suspected in gunshot injuries, as preoperative imaging is sometimes inconclusive. Before removal of the IOFB is attempted, complete removal of any vitreous condensations around the IOFB must be performed in order to ensure a smooth removal process, free of any traction on the retina. Traditional 20-gauge vitrectomy is advised in the situation of a suspected IOFB, as it is sometimes necessary to enlarge the sclerotomy in order to remove the IOFB (Figure 6).
An alternative is to use small-gauge valved trocars and create a fourth 20-gauge sclerotomy through which the IOFB is removed. The benefit of this technique is that, after removal of the IOFB, the sclerotomy can be sutured closed, and the small-gauge closed system can be maintained throughout the remainder of surgery. If the IOFB is too large to exit through a sclerotomy, it can be removed through a corneal incision after removal of the crystalline lens.
Retinal detachment renders the surgical procedure much more difficult. The causative break or breaks are usually not obvious due to the surrounding organized vitreous hemorrhage. Also, frequently due to the severe breakdown in the blood-ocular barrier, epiretinal fibrosis is encountered, and meticulous removal of these membranes necessary if the retina is to remain attached throughout the postoperative period (Figure 7).
The occurrence of epiretinal membranes (ERMs) and proliferative vitreoretinopathy (PVR) is much higher in gunshot wounds than in vitrectomies for other pathologies. Some surgeons favor internal limiting membrane (ILM) peeling at the time of the vitrectomy so as to remove the scaffold on which ERMs proliferate.
In the situation of a detached retina, it is also difficult to perform thorough shaving of the vitreous base. The organized hemorrhage at the periphery of the retina prevents the surgeon from clearly delineating the hemorrhage from the surface of the retina. Also, any iatrogenic breaks in this area will surely lead to a recurrence of the detachment. We advise that, with the assistance of scleral indentation, close but safe shaving of the vitreous base should be done, taking care not to injure the retina at its periphery.
At the end of the vitrectomy, after removal of the vitreous hemorrhage and the IOFB, the surgeon has to choose what to leave the vitreous cavity filled with (Figure 8). If there is no retinal detachment, then we would leave the eye filled with balanced salt solution. If the retina is detached, we would recommend choosing 5000 cSt silicone oil. This high viscosity oil is more resistant to emulsification than its lighter counterparts. Because we usually like to follow-up the retinal condition for a period of time longer than usual, this high viscosity oil is ideal. After 6 to 12 months, provided that the retina is stable, the silicone oil can be removed and a secondary IOL implanted in the sulcus.

Figure 9. Exit wound near the macula with dense submacular hemorrhage and a large posterior break.
WHAT TO EXPECT AND WHAT TO TELL THE PATIENT
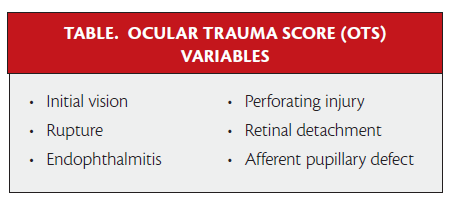
Visual prognosis following gunshot injuries to the globe depends on a number of key factors. The ocular trauma score (OTS), devised to help in predicting visual acuity outcomes after ocular trauma, is helpful but not entirely accurate in these situations (Table). The prognostic factors that have the greatest influence on visual outcomes after vitrectomy for gunshot injuries are the site of the exit wound, concurrent optic nerve injury, associated retinal detachment, and submacular hemorrhages. Even when visual acuity at the time of presentation is very poor (light perception), good postoperative visual outcomes can be achieved. Gunshot injuries are usually associated with dense vitreous hemorrhages that greatly affect vision (sometimes resulting in no light perception). When hemorrhages are removed, provided no other poor prognostic factors were present, vision can improve markedly.
Endophthalmitis is a devastating condition, but it is rarely seen in the setting of gunshot injuries. This is probably due to the heat generated by the firearm, rendering the pellets sterile.
In our opinion, the exit wound is the primary prognostic factor. If the exit wound involves the macula and/or the optic nerve, then visual outcomes are extremely poor, even after successful surgery (Figure 9).

Figure 10. Metallic foreign bodies lying in the vicinity of the optic canals of both eyes.
Optic nerve injury does not always occur because of an exit wound’s proximity to the nerve. In certain circumstances the pellet can find its way to the optic canal and cause optic nerve damage without an associated open globe injury (Figure 10). These are rare circumstances. Our theory on how this happens is that the pear-shaped anatomy of the orbit directs the pellet toward its stalk (ie, the optic canal), and the result is irreversible damage to the optic nerve.
Associated retinal detachment is another important prognostic factor. Even after successful flattening of the retina, visual acuity may remain poor. Retinal detachment can be of the rhegmatogenous, tractional, or mixed type. The track formed by the pellet as it moves through the eye organizes and becomes fibrosed. This organized track of vitreous, blood, and fibrous tissue exerts traction on the retina, causing it to detach. In other circumstances, even in the presence of an exit wound, the retina may remain attached.
CONCLUSION
Gunshot injuries to the eye are devastating. Trauma is sometimes bilateral and always severe. With sound planning and creative modifications of operative technique, anatomic success can be achieved in most cases. Visual prognosis depends on a number of key factors, and, with a little bit of luck, some form of functional vision can be restored for these patients. n
Omar A. Barrada, MD, is lecturer in the ophthalmology department of Cairo University Medical School (El Kasr El Aini). Dr. Barrada may be reached at omarbarrada@hotmail.com.
Mahmoud M. Soliman, MD, is is a professor of ophthalmology at Cairo University Medical School (El Kasr El Aini).
Ayman M. Khattab, MD, is a professor of ophthalmology at Cairo University Medical School (El Kasr El Aini).
1. Kuhn F, Morris R, Mester V, Witherspoon CD. Terminoogy of mechanical injuries: the Birmingham Eye Trauma Terminiology (BETT). In: Kuhn F, ed. Ocular Traumatology. New York: Springer; 2008:3-11.





_1784132761.jpg?auto=compress,format&w=75)











