
Proliferative vitreoretinopathy (PVR) can occur after cryopexy, laser retinopexy, pneumatic retinopexy, scleral buckling, or vitrectomy.1,2 The presence of an epiretinal membrane (ERM) following retinal detachment repair can be considered limited PVR, but the optimal timing for removal is not clear. When combined with a detachment, peeling the ERM in addition to the peripheral membranes is complex and crucial to the surgical outcome.
Fortunately, we have many different tools to identify and peel the membranes in addition to adjuvants to simplify the peeling process.3 Using the most appropriate tools in a step-wise fashion is important.
Case Report
A 67-year-old man experienced a sudden decrease in vision to hand motions in the right eye. Approximately 10 years previously, he experienced a retinal detachment in his left eye, which was managed with a scleral buckle. His family history included a retinal detachment in his father.
Eight months prior to the current presentation, the patient was found to have a giant retinal tear (GRT) extending from 12:00 to approximately 7:30 with the macula off. He underwent a scleral buckle, vitrectomy, laser, and oil at that time, given the extension of the GRT inferiorly. His retina remained flat and attached for 7 months before we considered oil removal.
During that time, a cataract progressed significantly, and a dense ERM developed. We debated removing the ERM at the time of oil and cataract removal but decided to simplify the surgery by removing only the oil and cataract. This surgery was performed without complication. The patient’s visual acuity following this surgery was 20/200.
Four weeks later, the patient presented with a sudden curtain across his vision in his right eye, and visual acuity had decreased to hand motions. On examination, he had a starfold temporally with a stretch hole at 9:30, and the retina was detached through the macula (Figure 1). He had a prior buckle in place following the GRT repair. Therefore, we planned a vitrectomy with a membrane peel, laser, and tamponade to be determined.
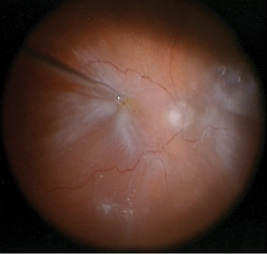
Figure 1. Intraoperative image of the initial presentation of the right eye demonstrating a retinal detachment with a dense epiretinal membrane.
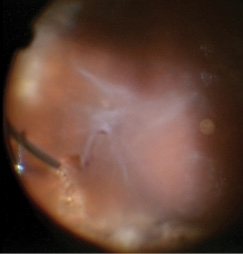
Figure 2. Intraoperative image of the starfold adjacent to the stretch hole in the temporal periphery.
Vitrectomy was performed under monitored anesthesia with a retrobulbar block of 50:50 2% lidocaine and 0.75% bupivacaine. Three self-retaining 25-gauge cannulas were placed with a beveled incision and conjunctival displacement. I performed the vitrectomy using the Constellation Vision System (Alcon) under a wide-field noncontact microscope system (Resight/Lumera 700, Carl Zeiss Meditec).
A small amount of diluted triamcinolone acetonide (Kenalog, Bristol-Myers Squibb) 1:3 was injected to stain the membranes associated with the starfold, as well as the ERM in the macula. Disposable internal limiting membrane (ILM) forceps were used to lift the edges of the membranes before switching to 25-gauge Grieshaber MaxGrip forceps (Alcon). The starfold temporally was difficult to fully peel given the presence of the stretch hole (Figure 2). Ultimately, I decided to create a draining retinotomy with the vitrector in that area, given its peripheral location, and to excise the starfold at the same time.
I turned my attention to the posterior pole. Indocyanine green (ICG) was used to stain the ILM (Figure 3), which was gently peeled using the MaxGrip forceps (Figure 4). This was followed by an air-fluid exchange using a soft-tip cannula (MedOne Surgical) taking care to remove all of the subretinal fluid through the draining retinotomy. The retina flattened nicely. Silicone oil (Silikon 1000, Alcon) was infused through the 25-gauge cannula for longer-term tamponade.
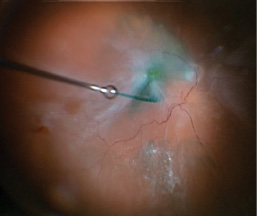
Figure 3. Intraoperative image showing the use of ICG to stain the ILM. Note the stretch hole in the periphery.
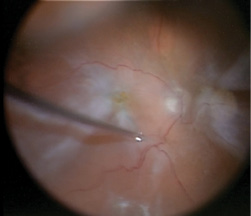
Figure 4. Intraoperative photo demonstrating the use of MaxGrip forceps to peel the ILM toward the posterior pole.
The retina remained flat for 2 months (Figure 5), and the patient’s pinhole visual acuity is 20/60.
Discussion
This case highlights the use of numerous tools to address the complex pathology in eyes with PVR detachments, as well as the benefits of using them in a step-wise approach. Individual staining of the premacular membranes and the ILM greatly enhanced visualization and allowed the complete removal of the ERM in the macula and the ILM. When the peripheral membranes could not be removed adequately, the use of the cutter to create a small retinectomy/draining retinotomy greatly simplified drainage and relieved the peripheral traction.
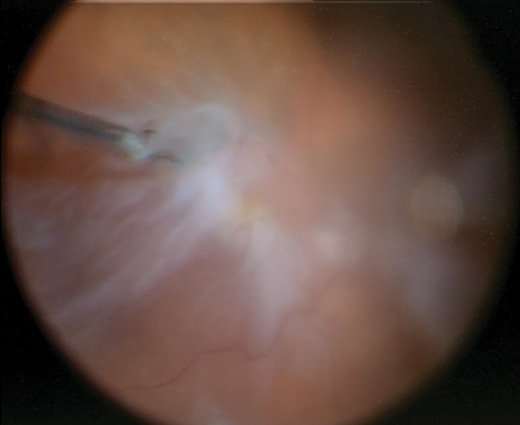
Figure 5. Intraoperative image of the ERM being regrasped at the base and peeled toward the stretch hole in the periphery.
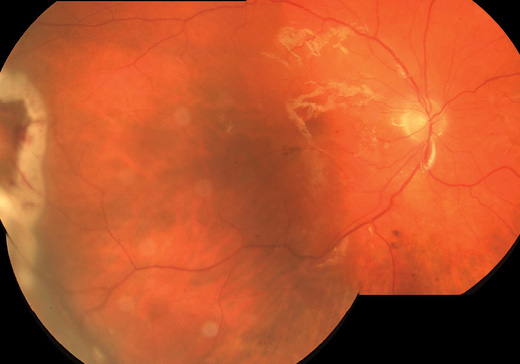
Figure 6. Color montage photo 1 week following surgery demonstrating the retina to be flat and attached under oil with the draining retinotomy/retinectomy in the temporal periphery.
The MaxGrip forceps provided the grip needed to gently peel the posterior pole premacular membranes from the surface of the retina. We debated the use of a heavy liquid to stabilize the macula and provide counter traction, but I found that with gentle, constant force directed toward the posterior pole and then toward the stretch hole, I could completely peel the ILM/ERM from the macular surface. Repeated regrasping at the base of the membrane minimized movement of the retina and allowed for maximum control of the removal of the posterior membrane in terms of force and direction (Figure 6).
While perfluorocarbon liquids are great tools in PVR detachments, they are not without risks.4,5 In cases like these, it is prudent to have access to heavy liquids, although I usually attempt to peel without them initially.
Conclusion
The enhancements in visualization systems, vitrectomy machines, surgical tools, and surgical adjuvants have revolutionized our ability to handle PVR detachments. n
Editorially independent supported by advertising from Alcon and Topcon.
1. Sethi CS, Lewis GP, Fisher SK, et al. Glial remodeling and neural plasticity in human retinal detachment with proliferative vitreoretinopathy. Invest Ophthalmol Vis Sci. 2005;46:329-342.
2. Rodriguez de la Rúa E, Pastor JC, Aragón J, et al. Interaction between surgical procedure for repairing retinal detachment and clinical risk factors for proliferative vitreoretinopathy. Curr Eye Res. 2005;30:147-153.
3. Young TA, D’Amico DJ. Controversies in proliferative vitreoretinopathy tamponade and pharmacologic adjuvants. Int Ophthalmol Clin. 2005;45:163-171.
4. Berrocal MH, Chenworth ML, Acaba LA. Management of giant retinal tear detachments. J Ophthalmic Vis Res. 2017;12:93-97.
5. Méndez-Martínez S, Calvo P, Rodriguez-Marco NA, et al. Blindness related to presumed retinal toxicity after using perfluorocarbon liquid during vitreoretinal surgery. Retina. 2017;Jul 18.
Geeta Lalwani, MD
• founder of Rocky Mountain Retina Associates in Boulder, CO
• no financial or proprietary interests in the products or companies discussed herein
• glalwani@RMRetina.com












