


Circumscribed choroidal hemangioma is a benign vascular tumor characterized in part by its red-orange hue. Associated findings include serous retinal detachment, overlying photoreceptor atrophy, cystoid macular edema, retinal pigment epithelial alterations, and subretinal fibrosis.1
Although choroidal hemangioma frequently manifests these distinct clinical features, it has often been confused with other chorioretinal abnormalities, such as macular edema, retinal detachment, central serous chorioretinopathy, choroidal melanoma, and choroidal metastases.1 Conversely, other pathologies can masquerade as choroidal hemangioma, specifically dome-shaped maculopathy.2
AT A GLANCE
- Circumscribed choroidal hemangioma is a benign vascular tumor with distinct clinical features such as a red-orange hue, subretinal fibrosis, overlying photoreceptor atrophy, and retinal pigment epithelial alterations.
- Choroidal hemangioma has been confused with macular edema, retinal detachment, and other chorioretinal abnormalities.
- The tessellated, red-orange appearance of extramacular dome-shaped elevation can clinically simulate a tumor such as choroidal hemangioma, but ancillary testing with EDI-OCT, FA, and ICGA may help distinguish this abnormality.
Here we present a case of extramacular dome-shaped elevation that was referred to our practice for suspicion of circumscribed choroidal hemangioma.
CASE REPORT
A 79-year-old Hispanic man with an ocular history of advanced open-angle glaucoma was referred to the Ocular Oncology Service at Wills Eye Hospital for suspicion of a choroidal tumor in the left eye. His medical and ocular histories included cataract surgery in the left eye, trabeculectomy and glaucoma tube shunt implantation in the left eye, diabetic retinopathy with macular edema in the left eye, left facial synkinesis, and left eyelid trauma. He reported no symptoms related to the choroidal lesion.
On examination, VA was light perception OD and 20/400 OS. There was a relative afferent pupillary defect in the right eye. IOP measured 22 mm Hg OD and 12 mm Hg OS. Anterior segment examination revealed no abnormalities except for the presence of the glaucoma tube shunt and a superior iridotomy in the left eye. No ocular melanocytosis or heterochromia was noted.
Fundoscopy revealed advanced cupping of the optic nerve and scattered intraretinal hemorrhages in both eyes, with macular edema in the left eye. Just inferior to the optic disc in the left eye, a red-orange lesion was noted, measuring 6 mm by 5 mm in basal diameter (Figure 1A). There was no abnormal autofluorescence
pattern noted overlying the lesion (Figure 1B).

Figure 1. Fundus photography shows a tessellated red-orange lesion inferior to the optic disc (arrows), measuring 6 mm by 5 mm in basal diameter; scattered intraretinal hemorrhages are more prominent superiorly (A). Fundus autofluorescence shows no abnormalities at the location of the lesion inferior to the optic disc (B).
B-scan ultrasonography demonstrated an apparent dome-shaped mass with solid echogenicity and a thickness of 2.3 mm (Figure 2A). There was no subretinal fluid (SRF) and no overlying vitreous abnormalities. Enhanced depth imaging OCT (EDI-OCT) revealed a dome-shaped elevation of the retina without SRF or choroidal neovascularization (Figure 2B). On EDI-OCT, scleral elevation without choroidal thickening could be noted. No related abnormalities were seen on fluorescein angiography (FA) or ICG angiography (ICGA) (Figure 3).

Figure 2. B-scan ultrasonography shows a 2.3 mm elevation of the solid lesion inferior to the optic disc (A). EDI-OCT over the lesion shows scleral elevation (arrows) rather than choroidal thickening. Normal retinal architecture was maintained over the lesion, and no SRF or edema was noted (B).
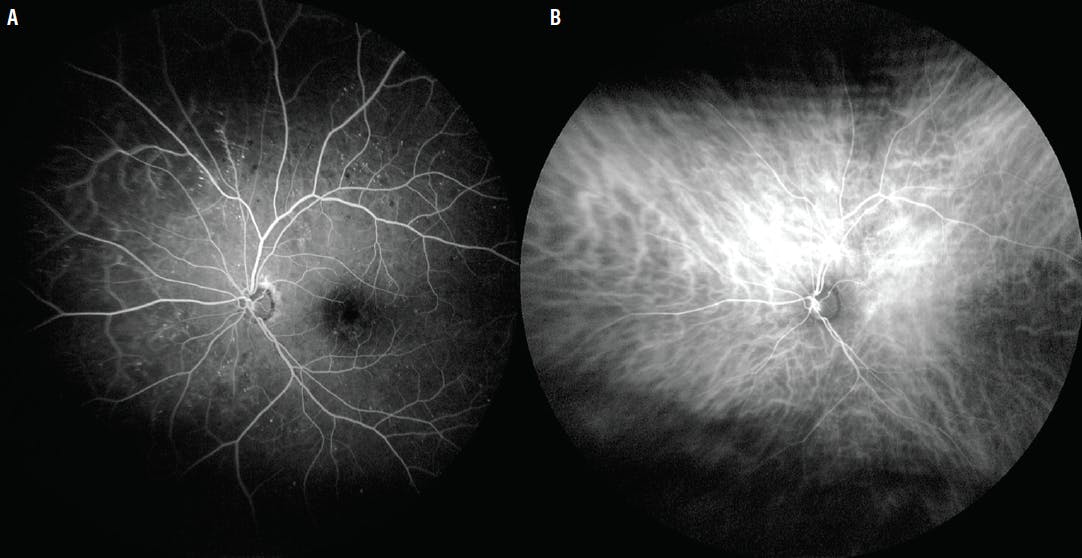
Figure 3. Fluorescein angiography shows scattered hyperfluorescent extramacular microaneurysms but no abnormalities over the lesion inferior to the optic disc (A). ICG angiography shows no abnormalities (B).
Ultimately, the clinical and imaging features suggested that the lesion was in fact not a tumor, but rather an extramacular dome-shaped elevation of the sclera that required no treatment and merited observation alone.
DISCUSSION
Dome-shaped maculopathy is a convex protrusion of the sclera, pushing the internal structures inward and occasionally simulating an intraocular tumor.2,3 Although most commonly associated with myopia or staphyloma, it has been reported in emmetropes and hyperopes as well.3 In an analysis of 58 eyes, Errera et al found that the mean refractive error associated with dome-shaped maculopathy was approximately -7.00 D.4 This condition can be found with other abnormalities, such as Best vitelliform macular dystrophy and oculocutaneous albinism.5,6 Additionally, EDI-OCT has confirmed that dome-shaped maculopathy is secondary to focal scleral thickening.2
In an analysis of 52 highly myopic eyes, Viola et al found that dome-shaped maculopathy was associated with serous retinal detachment (17 eyes, 33%), choroidal neovascularization (13 eyes, 25%), extrafoveal retinoschisis (two eyes, 4%), and lamellar macular hole (one eye, 2%).7 Further, 39 of the 52 eyes had a horizontally oriented oval-shaped dome, and 12 had a vertically oriented oval-shaped dome. Only one eye demonstrated a circular dome. Mean spherical equivalent in these eyes was -14.00 D and mean BCVA was 0.32 logMAR (Snellen equivalent of 20/40).7
In another study, Saito et al found that 37 of 82 eyes (45%) with a dome-shaped macula did not demonstrate a posterior staphyloma, indicating that dome-shaped maculae can develop independently from a posterior staphyloma.8
As its name suggests, dome-shaped maculopathy typically appears in the macula. However, extramacular dome-shaped elevation has been reported, and a similar pathophysiology to dome-shaped maculopathy has been theorized.9
The treatment strategy is targeted toward the management of SRF. In a retrospective case series by Lorenzo et al, 29 of 56 eyes demonstrated SRF at presentation. Of those 29 eyes with SRF, 10 eyes were observed without intervention. The other 19 eyes were managed with one of the following treatments: eight (42%) with low-fluence photodynamic therapy (PDT); seven (37%) with intravitreal bevacizumab (Avastin, Genentech), and four (21%) with intravitreal ranibizumab (Lucentis, Genentech). Resolution of SRF was seen in one (13%) of those treated with PDT (mean of 1.9 sessions), in one (14%) of those treated with intravitreal bevacizumab (mean of 1.9 injections), and in none (0%) of those treated with intravitreal ranibizumab (mean of 1.8 injections).
Overall, only four of the 29 eyes exhibited complete resolution of SRF, including one that received low-fluence PDT, one that received bevacizumab, and two that resolved spontaneously. The data show no statistically significant difference between eyes that were treated for SRF versus those that were not (P = .42).10
Burke et al also noted no difference in BCVA between eyes that received therapy and those that received no therapy (0.52 vs 0.45 logMAR, P = .19).3
In our patient, the fundus revealed a red-orange elevation with focal choroidal vascular tessellations that, at first glance, was concerning for choroidal hemangioma. Notably, however, the vascular pattern was normal. The dense echogenicity on ultrasonography would suggest either choroidal hemangioma or dome-shaped maculopathy. The most revealing points of differentiation were seen on EDI-OCT, FA, and ICGA, which excluded choroidal hemangioma because hemangioma would have demonstrated choroidal thickening with preservation of the choriocapillaris on EDI-OCT, hyperfluorescence with diffuse late staining on FA, and hypercyanescence with late wash-out on ICGA.2 Dome-shaped elevation typically shows normal fluorescence patterns other than staining when there is SRF.
CONCLUSION
Dome-shaped elevation of the sclera can occur in eyes with or without a history of myopia. The tessellated, red-orange appearance of extramacular dome-shaped elevation can clinically simulate a tumor such as choroidal hemangioma. Ancillary testing with EDI-OCT, FA, and ICGA may help distinguish this abnormality. In this case, observation alone was sufficient because of the lack of SRF or retinal edema.3
Support provided in part by the Eye Tumor Research Foundation, Philadelphia, PA (CLS). The funders had no role in the design and conduct of the study, in the collection, analysis and interpretation of the data, and in the preparation, review or approval of the manuscript. Carol L. Shields, MD, has had full access to all of the data in the study and takes responsibility for the integrity of the data.
1. Dalvin LA, Lim LAS, Chang M, et al. Circumscribed choroidal hemangioma. Clinical features and outcomes by age category in 458 cases. Saudi J Ophthalmol. 2019;33:219-228.
2. Iyer PG, Say EAT, Shields CL. Dome-shaped macula simulating choroidal hemangioma in a myopic patient. Oman J Ophthalmol. 2015;8(3):188-190.
3. Burke TR, Wu AD, Shen Y, Rajendram R. Longitudinal follow-up of dome-shaped macula. Eye (Lond). 2020;34(10):1903-1908.
4. Errera MH, Michaelides M, Keane PA, et al. The extended clinical phenotype of dome-shaped maculopathy. Graefes Arch Clin Exp Ophthalmol. 2014;252:499-508.
5. Parodi MB, Zucchiatti I, Fasce F, et al. Dome-shaped macula associated with Best vitelliform macular dystrophy. Eur J Ophthalmol. 2015;25(2):180-181.
6. Kumar V, Molla K, Chandra P, Kumar A. Dome-shaped macula in oculocutaneous albinism. BMJ Case Rep. 2016:bcr2016215368.
7. Viola F, Dell’Arti L, Benatti E, et al. Choroidal findings in dome-shaped macula in highly myopic eyes: a longitudinal study. Am J Ophthalmol. 2015;159(1):44-52.
8. Saito R, Shinohara K, Tanaka N, et al. Association between dome-shaped macula and posterior staphyloma in highly myopic eyes investigated by ultra-wide field optical coherence tomography [published online ahead of print 13 Jul 2020]. Retina.
9. Mutha V, Kumar A, Chawla R, Ravani RD. Extramacular dome-shaped elevation: a novel finding in a case of high myopia. BMJ Case Rep. 2017:bcr2017220861.
10. Lorenzo D, Arias L, Choudhry N, et al. Dome-shaped macula in myopic eyes: twelve-month follow-up. Retina. 2017;37(4):680-686.






_1784132761.jpg?auto=compress,format&w=75)










