

AT A GLANCE
- An audit of intravitreal injection management in one ophthalmology department yielded key ideas for improving capacity.
- Each department has its own problems and needs its own solutions. A given rule is not applicable everywhere, and outside help with organization is often needed.
- Regular reassessment is mandatory to maintain practice efficiency.
Our ophthalmology department is located in Seine-Saint-Denis, a suburb of Paris known for its high rate of unemployment, low salaries, and poor medical follow-up.1 There are 2 million people living in this area—almost the same as the population of Paris—but they are served by one-tenth the number of physicians. About 50% of patients in our catchment area do not speak French fluently. Our center mainly specializes in medical and surgical retina care, and we currently perform approximately 3,000 intravitreal injections (IVIs) per year.
In recent years, we have faced a large increase in demand for IVIs as the number of treatment indications has risen. During the summer of 2016 we modified the architecture of our IVI rooms to increase our IVI capacity without increasing staff numbers (Figure 1).

Figure 1. In our intravitreal injection area, two rooms were optimized (A, B) so that clinicians could access both rooms without exiting (black arrow shows route), while patients had two different entrances. A corridor was made available for patient preparation (C). The intravitreal area has its own waiting room.
Despite this physical alteration, we still faced organizational difficulties that limited the potential of our new rooms. Moreover, during this period the use of a treat-and-extend (TAE) regimen became the first-choice therapeutic strategy for most retinal diseases. This type of regimen, although it improves visual outcomes, also makes the organization of our IVI program much more complex.
In 2017, we had the opportunity to undergo an external audit of our procedures. This article outlines the outcomes of the audit, the changes our department made as a result, and the effect of those changes on our clinical efficiency within our IVI program.
BEFORE THE AUDIT
The idea of conducting an audit was suggested by Allergan, which then helped us to fund the audit. An auditor spent two consecutive days in our department and observed our organization (or, rather, disorganization).
At that time, patients had to wait for hours. One physician was responsible for performing IVIs and another handled the clinical assessment of patients following the TAE regimen; however, these IVI patients were clinically assessed in the middle of a general clinical practice. Patients had only one appointment, regardless of their regimen. During a TAE follow-up visit, patients did not understand why their IVI was performed long after the time of their clinic appointment.
The auditor interviewed every person involved in IVI administration and held two meetings to collect feedback from all professionals regarding the organization of IVIs. The auditor also helped us to develop a satisfaction scale to assess the reactions of our patients treated with IVIs.
RESULTS OF THE AUDIT
The auditor identified the following points:
- We often did not offer a TAE regimen to our patients (< 10% of cases) due to the organizational difficulties.
- Orthoptists and physicians were dedicated to multiple tasks: that is, to general clinical practice and performing IVIs at the same time.
- The list of patients and the eyes to be treated (OD, OS, or both) was verified on the same morning the IVIs were scheduled.
- We participated in multiple clinical trials with differing follow-up protocols.
The auditor found that the staff was dissatisfied with the organization but was very sensitive to the audit process. The patient survey showed that 40% of patients had to wait more than 1 hour to receive their IVI, regardless of the type of regimen they received, with a mean total time of 45 minutes in our department.
On a 6-point scale, with 1 corresponding to “completely satisfied” and 6 corresponding to “very dissatisfied,” our department earned an overall satisfaction score of 4 from our patients (Figure 2).
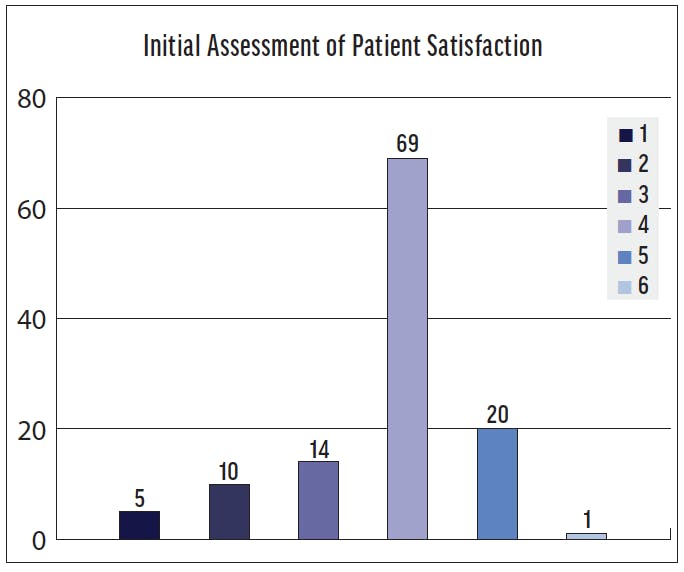
Figure 2. This chart shows the assessment of patient satisfaction regarding time spent in the clinic prior to the audit, based on a scale of 1 to 6 (1, completely satisfied; 2, very satisfied; 3, satisfied; 4, not quite satisfied; 5, not satisfied at all; 6, very dissatisfied).
After this observation phase, the auditor suggested several ways to change our IVI management approach:
- Improve the use of our own staffing resources (residents, nurses, orthoptists).
- Optimize patient flow (the main goal), including flow direction and appointment scheduling.
- Improve our department’s visibility and the patient information provided.
Specifically, the auditor recommended dedicating two clinicians to the intravitreal activity at the start of an IVI session but then assigning different tasks thereafter. There would be two practitioners to conduct the BCVA measurement and OCT scans at the start of a session, and then after 30 minutes one of them would be dedicated to those tasks and the other one dedicated only to the IVI procedure itself.
The auditor also advised that we schedule two appointments for each patient: one for measuring BCVA and performing OCT, and another one 30 minutes later for the IVI. The list of appointments for BCVA measurement and OCT would be scheduled to start 30 minutes before the list of IVI appointments.
These measures aimed to reduce patient waiting time, increase the number of injections performed, increase the number of patients followed with a TAE regimen, and achieve a good balance between the number of IVIs performed and the number of appointments.
The auditor also recommended that we verify patient charts the day before, rather than the morning of, the IVI sessions to ensure starting on time.
RECOMMENDATIONS APPLIED
We implemented several changes based on the recommendations of the auditor:
- We created two scheduling lists starting 30 minutes apart for patients treated with a TAE regimen: one for measuring BCVA and performing OCT and another for the IVI session.
- We scheduled two appointments for patients treated with a TAE regimen.
- We dedicated two health care professionals to the BCVA measurement and OCT scans, and then, 30 minutes later, their tasks were split between those tasks and performing the IVI (apart from the general clinical practice), with the IVI scheduled later during the session.
- We verified IVI lists the day before the session instead of that morning.
We made these changes in March 2017 and then reassessed our practice that November. We found that the number of IVIs performed had increased, and we were able to propose a TAE regimen to more patients (50% vs < 10%). These changes allowed us to improve our IVI capacity by 30% between 2016 and 2019 (Figure 3).
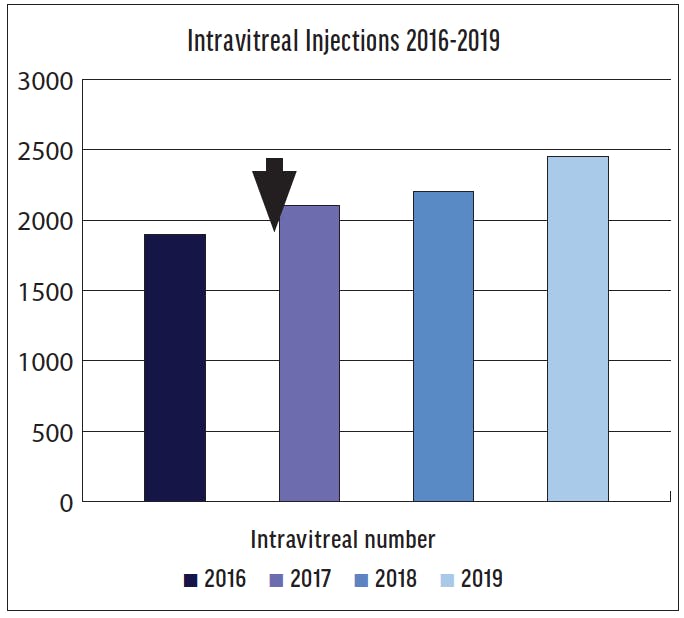
Figure 3. This chart depicts the number of intravitreal injections performed annually in the department during the past few years. The arrow indicates the date of the audit.
However, the overall time that patients spent in the clinic did not decrease (mean 45 minutes in March vs 44 minutes in November).
We tested and applied these recommendations within the constraints of a public hospital, which included insufficient numbers of health care practitioners (orthoptists, physicians, nurses), a large number of medical students, and frequent turnover of practitioners.
THREE YEARS LATER
We recently participated in a European meeting on the optimization of IVI capacity in retina departments, and this provided a good opportunity to assess our practice 3 years after the audit. In reviewing our performance, we noted that our use of the TAE regimen had recently decreased.
We recognized that the changes implemented after the 2017 audit were no longer being followed. These practices had lapsed due to the regular turnover among practitioners, including residents, nurses, and schedulers.
As a result of the reassessment, we decided to once again reorganize our scheduling and other practices as recommended by the auditor. This experience helped us to understand that regular reassessment is mandatory to maintain efficiency in practice.
CONCLUSION
Even though we improved our local IVI capacity by 30% over the past 3 years, we did not reduce the mean overall time patients spent in our clinic. Still, we were able to increase the number of patients treated with a TAE regimen and to formalize this type of regimen with two appointments, which has helped to increase patient satisfaction.
We also realized through this audit experience that each department has its own problems and requires its own solutions. A given rule is not applicable everywhere, and small changes can make a big difference.
1. Stéphan S, Fajnkuchen F, Addou-Regnard M, et al. Severity of diabetic macular edema (DME) in Seine St Denis among patients treated by anti-VEGF [in French]. J Fr Ophtalmol. 2014;37(9):717-721.



_1784132761.jpg?auto=compress,format&w=75)











