

AT A GLANCE
- The indications for autologous retinal transplantation (ART) have expanded as surgeons become more adept at the procedure.
- Before and at the time of perfluorocarbon liquid removal, it is essential to recognize slight graft displacement, occurring in approximately 10% of ART cases.
- In the authors’ experience, delayed retinal detachments occurring weeks after the ART are not associated with a dislocation, as the graft is already integrated within the retina; thus, surgeons can focus on fixing the detachment.
The closure rate for primary macular holes (MHs) after pars plana vitrectomy (PPV) and internal limiting membrane (ILM) peel is excellent, but sometimes a refractory or atypical hole requires a more aggressive surgical technique. Autologous retinal transplantation (ART) can be a successful primary surgical option in patients with a large, chronic, or atypical MH. Additionally, it can be a secondary surgical option in patients with a refractory MH after PPV with ILM peel or ILM flap.1-5
The indications for ART have been expanding as surgeons become more adept at the procedure. For example, ART in combination with autologous retinal pigment epithelium and choroid transplantation can successfully close a chronic MH with underlying geographic atrophy and/or subretinal fibrosis.6 Additionally, ART can be used to treat refractory optic disc coloboma–associated serous retinal detachments.7
The theoretical advantage of ART is that the transplanted retina will integrate into the adjacent tissue, potentially improving visual recovery compared with other inert tissue scaffolds.8,9 In the Global Consortium Study, 33 vitreoretinal surgeons validated the feasibility of this procedure, achieving a high MH closure rate and good visual recovery in patients undergoing ART.3 Nevertheless, surgical difficulties and complications of ART persist, including perfluorocarbon liquid (PFCL)-specific complications, graft dislocation, and retinal detachment.
PFCL PITFALLS
Intraoperatively, the use of PFCL is crucial to stabilize the retina during graft harvesting, manipulation, and placement in the bed of the MH. PFCL can be left in the eye as a short-term tamponade (1 to 2 weeks) to secure the graft and allow easier patient positioning (flat on the back). There is also a theoretical improvement in oxygen diffusion through a PFCL-filled vitreous cavity, which may have implications for early graft perfusion.10 However, a separate surgery for PFCL removal is required as long-term PFCL retention is associated with intraocular inflammation.
Before and at the time of PFCL removal, it is essential to recognize slight graft displacement (as opposed to dislocation), occurring in approximately 10% of ART procedures.3 If an eccentrically displaced graft is noted before PFCL removal, an adjustment can be performed. Although ILM forceps can be used for this, the Finesse Flex Loop (Alcon) may serve as a useful tool to gently manipulate the ART in the direction of the eccentric displacement under PFCL (Figure 1). After the adjustment, PFCL-air exchange with subsequent intraocular gas exchange is appropriate.

Figure 1. OCT demonstrates an eccentric ART with a nasal opening (A). Intraoperative photographs document before (B) and after (C) an adjustment of the ART. The post-adjustment OCT demonstrates good closure (D).
A dreaded complication of PFCL use is subretinal PFCL, reported in up to 11% of cases in which PFCL was used during vitreoretinal surgery in general.11 The incidence of subretinal PFCL in the Global Consortium Study was significantly less, at 1.5%, and occurred only when ART was used to treat a combined MH-rhegmatogenous retinal detachment.3
The high specific gravity of PFCL that makes it useful in vitreoretinal surgery is also the property that results in its subfoveal migration. Therefore, in the event of subfoveal PFCL after ART, it is imperative to completely remove the PFCL to preserve the integrity of the retinal graft. Although many techniques for removal of subfoveal PFCL have been described, including the use of a small-gauge (39- or 41-gauge) cannula, these approaches are not advised in ART because they could lead to dislocation of the recent transplant. Instead, the following steps can be employed to remove PFCL bubbles under the ART:
- Completely remove PFCL from the vitreous cavity using a backflush soft-tip cannula with the eye tilted toward the optic disc.
- Visualize the subfoveal PFCL bubbles under the ART (Figure 2).
- With the backflush soft-tip cannula, apply gentle pressure over the ART to extrude the bubbles through the transplant edge to the preretinal space.
- Tilt the eye toward the optic disc and remove the bubbles with passive aspiration away from the ART.
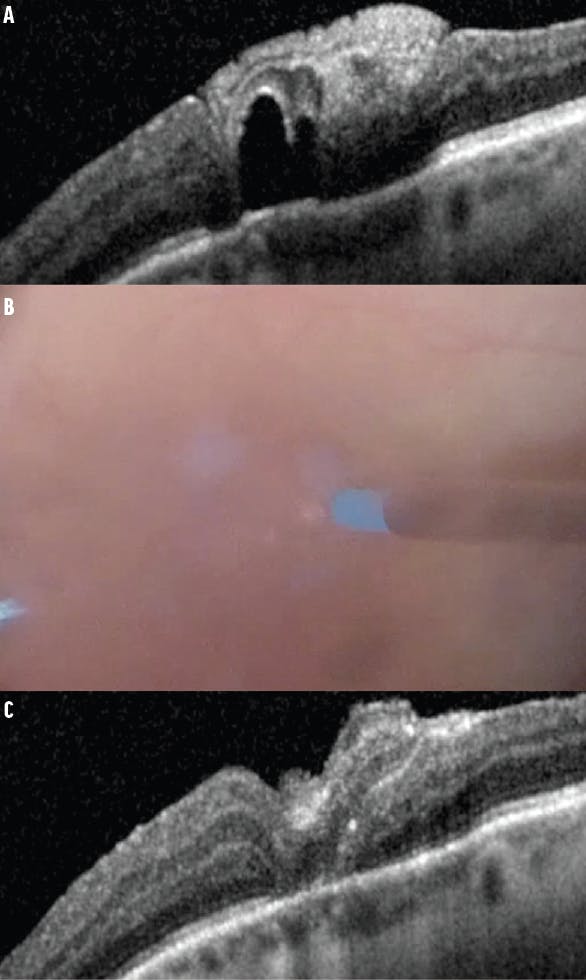
Figure 2. OCT imaging reveals subretinal PFCL after ART (A). During the procedure, gentle pressure is applied to the ART to express the PFCL bubbles around the graft (B). Postoperative OCT shows successful removal of the subretinal PFCL (C).
This technique is highly successful because the fresh transplant has not yet fully integrated within the adjacent macular tissue, allowing a path of minimal resistance for the PFCL bubbles to egress.
GRAFT DISLOCATION
Complete graft dislocation occurs in 3.8% to 4.8% of ART cases, necessitating a second surgery to repair the MH.2,3 In the event of a graft dislocation, one can consider placing the subsequent ART in the subretinal space. Although the Global Consortium Study showed no statistically significant improvement in MH closure or visual acuity with a subretinal ART versus a preretinal ART,3 we recommend placing the second ART in the subretinal space to help minimize the chances of a second dislocation.
One of the difficulties with subretinal ART placement is the bimanual manipulation that is often required. Before attempting bimanual subretinal placement, the surgeon can use PFCL to place the ART in the subretinal space (Figure 3). With PFCL in the backflush line, the surgeon can actively inject a small PFCL bubble over the ART to forcefully position the ART in the subretinal space.

Figure 3. This intraoperative photograph illustrates the use of PFCL to displace an ART in the subretinal space (A). The postoperative OCT shows successful closure (B).
RETINAL DETACHMENT
The risk of proliferative vitreoretinopathy (PVR) secondary to graft harvesting is a concern with ART. Fortunately, the incidence of a PVR retinal detachment after ART is low, occurring in only 3.8% of patients in the Global Consortium Study.3 If a PVR detachment occurs after a successful ART, standard vitreoretinal surgical techniques can successfully repair the detachment. However, care must be taken to protect the prior ART to prevent a displacement, dislocation, or both. To avoid this complication, PFCL should be used early in the detachment repair to reposit the displaced ART and stabilize the graft during more aggressive maneuvers.
In our experience, delayed detachments occurring weeks after an ART are not associated with a dislocation, as the graft is already integrated within the retina; thus, the surgeon can focus on fixing the detachment. However, a delayed PVR detachment with graft displacement can occur (Figure 4). Once PFCL is injected to reposit the ART, the retina can be successfully attached with excellent stability of the ART.
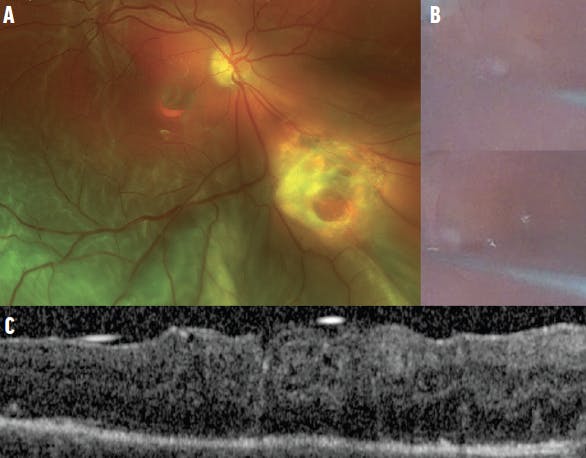
Figure 4. The fundus photograph shows a post-ART PVR detachment with a dislodged ART that is only partially closing the MH (A). The intraoperative photographs demonstrate the use of PFCL to reposit the ART (B). The postoperative OCT shows excellent ART placement (C).
CONCLUSION
ART can be a useful technique in the repair of atypical, recurrent, and combined retinal detachment–associated MHs. Although it is a complex surgical technique, it is associated with excellent results in most cases.
1. Grewal DS, Mahmoud TH. Autologous neurosensory retinal free flap for closure of refractory myopic macular holes. JAMA Ophthalmol. 2016;134(2):229-230.
2. Grewal DS, Charles S, Parolini B, Kadonosono K, Mahmoud TH. Autologous retinal transplant for refractory macular holes: Multicenter International Collaborative Study Group. Ophthalmology. 2019;126(10):1399-1408.
3. Moysidis SN, Koulisis N, Adrean SD, et al. Autologous retinal transplantation for primary and refractory macular holes and macular hole retinal detachments: the Global Consortium. Ophthalmology. 2021;128(5):672-685.
4. Tanaka S, Inoue M, Inoue T, et al. Autologous retinal transplantation as a primary treatment for large chronic macular holes. Retina. 2020;40(10):1938-1945.
5. Thomas AS, Mahmoud TH. Subretinal transplantation of an autologous retinal free flap for chronic retinal detachment with proliferative vitreoretinopathy with and without macular hole. Retina. 2018;38(Suppl 1):S121-S124.
6. Parolini B, Grewal DS, Pinackatt SJ, et al. Combined autologous transplantation of neurosensory retina, retinal pigment epithelium, and choroid free grafts. Retina. 2018;38(Suppl 1):S12-S22.
7. Temmerman IM, Mahmoud TH, Veckeneer MAH. Autologous neurosensory retinal transplant to treat refractory serous retinal detachment secondary to optic disc coloboma. Preprint. Published online June 17, 2020. Retina Cases Brief Rep.
8. Patel SN, Mahmoud TH, Kazahaya M, Todorich B. Autologous neurosensory retinal transplantation: bridging the gap. Preprint. Published online May 2, 2021. Retina.
9. Tabandeh H. Vascularization and reperfusion of autologous retinal transplant for giant macular holes. JAMA Ophthalmol. 2020;138(3):305-309.
10. Lowe KC. Perfluorocarbons as oxygen-transport fluids. Comp Biochem Physiol A Comp Physiol. 1987;87(4):825-838.
11. Garcia-Valenzuela E, Ito Y, Abrams GW. Risk factors for retention of subretinal perfluorocarbon liquid in vitreoretinal surgery. Retina. 2004;24(5):746-752.


-1_1638377570.jpg?auto=compress,format&w=70)




_1784132761.jpg?auto=compress,format&w=75)










