

Diabetes has been labeled an epidemic for 15 years—at least—and its ocular complications are simply unavoidable in a retina practice. If left unchecked, diabetic retinopathy (DR) can cause catastrophic vision loss.1 Despite a robust armamentarium of treatment options, DR remains the No. 1 cause of blindness in working-age adults in industrialized countries.2
Making matters worse, the demographics of this systemic disease are shifting. Historically, patients with type 2 diabetes were in their 40s; now, more and more of these patients are in their 20s and 30s.3 Some are even in adolescence.4 This poses a whole new set of problems because young eyes behave differently from aging eyes. For example, young eyes with signs of DR usually present with an attached hyaloid—and “the hyaloid is the enemy,” as María H. Berrocal, MD, reminds us in this issue. In her experience, she tells us, the status of the hyaloid to some degree dictates a patient’s risk for progression and complicates the treatment options.
Of course, diabetic eye disease is something we should be able to prevent with the therapies and surgical techniques at our disposal. Unfortunately, myriad factors interfere with a timely diagnosis, and even when they are diagnosed, patients with this chronic disease are notoriously lost to follow-up. Remember those young patients with diabetes? They are often reluctant to take time off from work and family to traipse into a specialist’s office just to hear, “Everything looks good, see you next year!” That is, until we catch something, and by then it’s often too late—the damage is done.
So researchers and clinicians continue to explore novel approaches to both the diagnosis and management of diabetic eye disease with a focus on early intervention and long-term stability.
In this issue of Retina Today, we look at some promising tools to help identify the first signs of retinopathy, including remote screening using deep-learning algorithms and ultra-widefield imaging to assess the retinal periphery.
When it comes to treatment, we have a lot to consider. Safer techniques and 27-gauge tools have made early vitrectomy an important consideration worth investigating in a randomized surgical trial. Intravitreal anti-VEGF injections have become a mainstay of treatment, and researchers are even exploring the potential impact of prophylactic anti-VEGF injections. The 2-year results of the DRCR Retina Network’s Protocol W study suggest some benefit of preventive treatment, and we are all eager to see the 4-year results.
Regardless of how you choose to integrate these advances into your clinical care routines, one thing is certain: When it comes to caring for patients with diabetes, earlier is better. The sooner we identify changes, the sooner we can intervene—one way or another—and preserve vision.
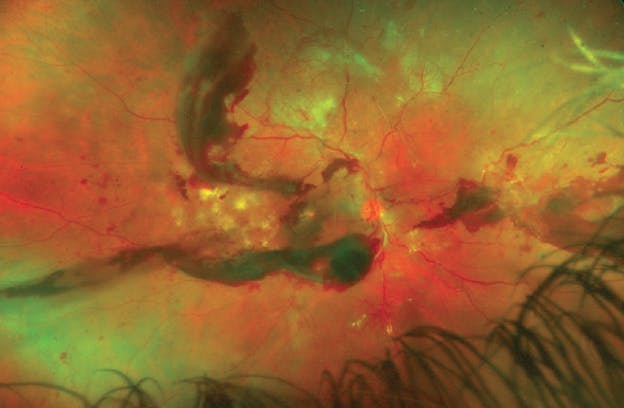
María H. Berrocal, MD, author of "The Benefits of Early Surgical Intervention For Diabetic Retinopathy," saw this 37-year-old patient with type 1 diabetes who presented with vitreous hemorrhage. Although he was scheduled for vitrectomy, he missed his appointment due to the COVID-19 pandemic. Read her article to see what this eye looked like when he returned 8 weeks later.
1. Bassett MT. Diabetes is epidemic. Am J Public Health. 2005;95(9):1496.
2. Guariguata L, Whiting DR, Hambleton I, et al. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin Pract. 2014;103(2):137-149.
3. Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of diabetes and its burden in the United States. 2017. Accessed June 3, 2021. www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
4. Centers for Disease Control and Prevention. A snapshot: diabetes in the United States. Accessed June 3, 2021. www.cdc.gov/diabetes/library/socialmedia/infographics/diabetes.html






_1784132761.jpg?auto=compress,format&w=75)











