


Coats disease is an idiopathic, nonhereditary retinal vascular disorder manifesting with telangiectasia, exudation, retinal detachment (RD), and potential risk for neovascular glaucoma and phthisis bulbi. It typically presents in children (mean age of onset is 5 years), more often in boys (> 75% of cases), and can lead to blindness.1-3 Although historically considered a unilateral disease, a 2019 report on 175 patients with Coats disease altered our understanding of the condition, revealing that asymptomatic retinal vascular abnormalities occurred in the fellow eyes of 19% of patients, including telangiectasia, aneurysms, segmental nonperfusion, leakage, and vascular tortuosity.4 So, what else is new? Herein, we discuss a case of Coats disease and explore newly published findings on this condition.
CASE REPORT
A 14-year-old male patient noted blurred vision in his left eye for more than 3 weeks. He was found to have macular exudation and referred to our ocular oncology clinic for evaluation.
On examination, VA was 20/20 OD and 20/200 OS. The right eye was normal. The left eye had a normal anterior segment and IOP; fundus evaluation showed prominent macular and circumpapillary exudation and shallow subretinal fluid (SRF). Peripheral retinal evaluation disclosed a localized inferotemporal region of intense retinal telangiectasia and light-bulb micro- and macroaneurysms, surrounded by exudative RD. OCT documented macular detachment, intraretinal and subretinal exudation, and cystoid macular edema, further confirmed on ultrasonography demonstrating a shallow RD. Fluorescein angiography (FA) revealed extensive telangiectasia and aneurysms along the entire temporal periphery and concentrated inferotemporally, all with peripheral nonperfusion, consistent with Coats disease (Figure 1).
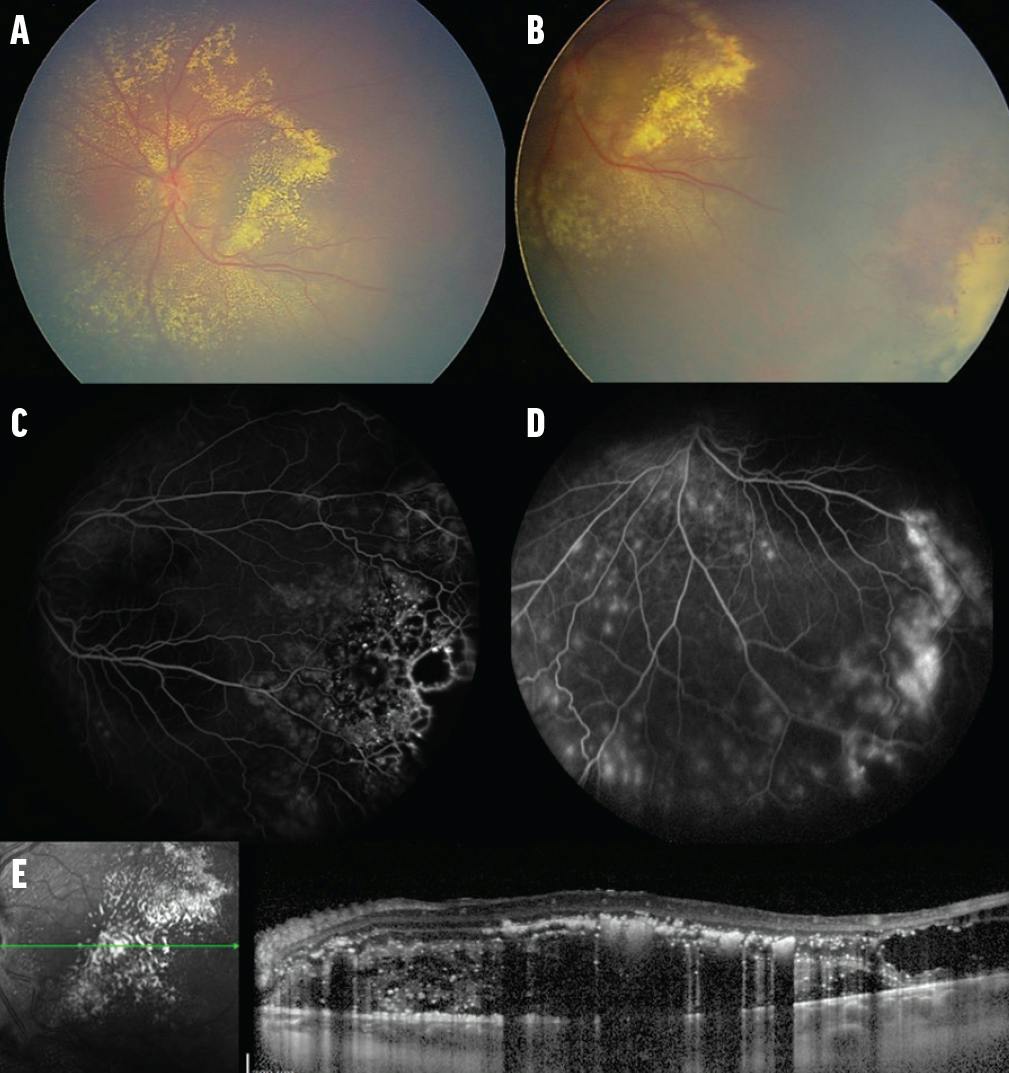
Figure 1. Coats disease at presentation (A). A 14-year old male patient with Coats disease in the left eye and VA of 20/200 presented with subretinal exudation in the posterior segment of the eye, including the macula (B). A region of intense retinal telangiectasia, light-bulb aneurysms, and nonperfusion was noted in the inferotemporal periphery (C), confirmed on FA (D) with leakage in later frames. OCT demonstrated subretinal and intraretinal fluid and exudation in the macula (E).
Treatment included laser photocoagulation for the less dense telangiectasia and cryotherapy for the denser macroaneurysms and retinal vascular abnormalities. Sub-Tenon corticosteroid injection of 10 mg (0.25 cc) was delivered to reduce inflammation. At 2 months, additional laser photocoagulation was provided to leaking telangiectasia. At 4 months, VA had improved to 20/40 OS, and the macular SRF, edema, and exudation had resolved, leaving a flat retina with minimal exudation (Figure 2).

Figure 2. Coats disease after treatment (A). Six months after treatment with cryotherapy and argon laser photocoagulation, there was remarkable improvement of subretinal exudation, leaving a flat retina, minimal residual exudation, and a chorioretinal scar in the inferotemporal periphery (B). This was confirmed by FA and OCT (C), which documented resolution of macular edema and residual intraretinal exudation. VA returned to 20/40.
DISCUSSION
There have been several changes in the diagnostic and therapeutic approaches since Coats disease was first described in 1908.5 In 2001, Shields et al classified Coats disease into five stages based on clinical features in 150 consecutive cases, ranging from asymptomatic retinal telangiectasia (stage 1), to telangiectasia with exudation (stage 2: 2A without macular involvement and 2B with macular involvement), exudative RD (stage 3: 3A1 with subtotal exudative RD sparing the fovea, 3A2 extending to the fovea, and 3B with total exudative RD), total RD with secondary glaucoma (stage 4), and end-stage disease with phthisis bulbi (stage 5).2
In that analysis, treatment options varied, with observation or laser photocoagulation for stage 1, laser photocoagulation or cryotherapy for stages 2-3A, cryotherapy for stage 3B with shallow RD, and surgical repair for stage 3B with bullous RD.2,3,5 Some cases of stage 4 disease with ocular pain required enucleation, and stage 5 cases usually required only observation.2,3,5 Visual outcomes also varied, with poor VA (20/200 or worse) in 0% of eyes with stage 1, 30% with stage 2A, 86% with stage 2B, 70% with stage 3A1 or 3A2, 94% with stage 3B, and 100% with stage 4 or 5.2
What About the Fellow Eye?
Although Coats disease has been considered a unilateral disease, vascular changes with uncertain clinical significance have been documented by FA in the fellow eye. Jeng-Miller et al recently studied 350 eyes of 175 patients and found that 19% had peripheral fellow eye abnormalities, consisting of telangiectasias (42%), aneurysms (55%), segmental nonperfusion (18%), leakage (18%), and diffuse vessel tortuosity (6%).4 These abnormalities were asymptomatic, remained unchanged during a mean follow-up of 25 months, and did not impact visual acuity. These authors questioned that Coats disease might represent a bilateral condition with asymmetric severity.4
What About Age of Onset?
Dalvin et al investigated the clinical features and outcomes of Coats disease by age and categorized patients as infant/toddler (≤ 3 years), child (> 3 to 10 years), or adolescent/adult (> 10 years). Comparison by age group revealed that the infant/toddler age group had worse presenting visual acuity; more anterior segment findings of xanthocoria, strabismus, and iris neovascularization (NVI); and more advanced disease stage.6 The youngest patients also had worse final visual acuity, experienced less complete disease resolution, and were more likely to be treated with primary enucleation.6
Daruich et al studied 98 patients in 2018 and confirmed more severe disease with younger age of diagnosis, as well as more evident leukocoria and strabismus; greater clock hour extent of peripheral retinal nonperfusion and telangiectasia; more foveal involvement; greater requirement for enucleation; and poorer final visual acuity.7
ANY TRENDS OVER THE PAST 50 YEARS?
Shields et al evaluated 351 cases of Coats disease over 45 years and classified the disease per decade from the 1970s to the 2010s. They found significantly more advanced Coats disease in the 1980s, including greater mean clock hours of exudation, as well as greater prevalence of four quadrants of exudation, four quadrants of SRF, and total exudative RD.5 They also found that treatment strategies have changed, with greater use of laser photocoagulation, sub-Tenon corticosteroid injection, and intravitreal anti-VEGF therapy in the 2010s, with less need for primary enucleation.5
Does the Amount of SRF Matter?
Failed resolution of SRF after treatment is considered to be a predictor of poor visual outcomes (< 20/200).2 Khoo et al studied 177 patients with RD in Coats disease and found that factors predictive of SRF resolution included absence of NVI on FA and less SRF elevation by ultrasonography.8 With each 1-mm decrease in SRF, the likelihood of SRF resolution increased by 16%.8
What’s the Risk for Enucleation?
When conservative therapies fail, patients with Coats disease can develop secondary glaucoma or pthisis bulbi and may require enucleation of the affected eye. Udyaver et al studied 259 eyes with Coats disease and found that predictors of enucleation included presence of NVI, ultrasonographic RD, open funnel RD, closed funnel RD, increasing ultrasonographic elevation of SRF by millimeters, and increasing angiographic extent of light-bulb aneurysms.9 Each 1-mm increase in SRF on ultrasonography increased the risk for enucleation by 20%, and each additional clock hour of light-bulb aneurysms by angiography increased the risk by 35%.9
Can We Predict Visual Outcomes?
In 2001, Shields et al found the most important predictive factors for poor visual outcome (< 20/200) included non-White race, diffuse disease, postequatorial and superior locations of telangiectasia and exudation, unresolved exudation after treatment, and the presence of retinal macrocysts.2
In 2019, Shields et al studied visual acuity outcomes in 160 patients with Coats disease who underwent Snellen visual acuity measurements before and after treatment. Using the stage at diagnosis, they found that advanced stage was associated with worse presenting VA (< 20/200; P < .001) and greater number of clock hours of telangiectasia, light-bulb aneurysms, exudation, and SRF.10 Patients with more advanced disease stage at diagnosis were also more likely to be treated with primary enucleation (P < .001) and had worse final VA (< 20/200; P < .001), typically from macular scar or persistent RD.10
CLINICAL TAKEAWAYS
The recent literature shows that Coats disease may be a bilateral condition with asymmetric involvement, and that younger age at presentation correlates with worse prognosis. Over the past 50 years, disease severity at presentation and diagnostic and therapeutic approaches have changed. Some presenting features can be predictive of SRF fluid resolution and risk for enucleation and can be used for prognosis.
Support provided in part by the Eye Tumor Research Foundation, Philadelphia, PA (CLS). The funders had no role in the design and conduct of the study, in the collection, analysis and interpretation of the data, and in the preparation, review or approval of the manuscript. Carol L. Shields, MD, has had full access to all the data in the study and takes responsibility for the integrity of the data.
1. Shields JA, Shields CL. Review: Coats disease: the 2001 LuEsther T. Mertz lecture. Retina. 2002;22(1):80-91.
2. Shields JA, Shields CL, Honavar SG, Demirci H, Caer J. Classification and management of Coats disease: the 2000 Proctor lecture. Am J Ophthalmol. 2001;131(5):572-583.
3. Shields JA, Shields CL, Honavar SG, Demirci H. Clinical variations and complications of Coats disease in 150 cases: the 2000 Sanford Gifford memorial lecture. Am J Ophthalmol. 2001;131(5):561-571.
4. Jeng-Miller KW, Soomro T, Scott NL, et al. Longitudinal examination of fellow-eye vascular anomalies in Coats’ disease with widefield fluorescein angiography: a multicenter study. Ophthalmic Surg Lasers Imaging Retina. 2019;50(4):221-227.
5. Shields CL, Udyaver S, Dalvin LA, et al. Coats disease in 351 eyes: analysis of features and outcomes over 45 years (by decade) at a single center. Ind J Ophthalmol. 2019;67(6):772-783.
6. Dalvin LA, Udyaver S, Lim LS, et al. Coats disease. Clinical features and outcomes by age category in 351 cases. J Pediatr Ophthalmol Strabismus. 2019;56(5):288-296.
7. Daruich A, Matet A, Munier FL. Younger age at presentation in children with Coats disease is associated with more advanced stage and worse visual prognosis: a retrospective study. Retina. 2018;38(11):2239-2246.
8. Khoo CTL, Dalvin LA, Lim LS, et al. Factors predictive of subretinal fluid resolution in Coats disease: analysis of 177 eyes in 177 patients at a single center. Asia Pac J Ophthalmol. 2019;8(4):290-297.
9. Udyaver S, Dalvin LA, Lim LS, et al. Predictors of enucleation in Coats disease: analysis of 259 eyes from 259 patients at a single center. J AAPOS. 2019;23(5):266.e1-266.e9.
10. Shields CL, Udyaver S, Dalvin LA, et al. Visual acuity outcomes in Coats disease by classification stage in 160 patients. Br J Ophthalmol. 2019;104(3):422-431.






_1784132761.jpg?auto=compress,format&w=75)










