


Lung cancer is the leading cause of cancer-related deaths for both men (22%) and women (22%) in the United States.1 Small cell lung cancer (SCLC) represents only 15% of all lung cancer cases, and nearly 70% of patients with SCLC present with disseminated disease upon diagnosis, which denotes a poor prognosis.2 Metastasis from any lung cancer most commonly affects the bone (59%), lymph nodes (50%), liver (41%), and brain (32%).3
In 2018, Shields et al reported that uveal metastases most often originate from cancer of the breast (37%) or lung (26%), and those from the lung have the poorest 5-year survival rate (13%) following detection of metastasis in the eye.4 Most intraocular metastases arise in the choroid (88%) and less commonly in the iris (9%) or ciliary body (2%).5
Herein, we describe a patient with known SCLC who developed photophobia from hyphema as the initial manifestation of metastasis to the iris.
CASE REPORT
A 66-year-old White man with a 14-month history of SCLC and known metastasis to the brain, bone, and liver presented to his primary care physician for photophobia in each eye, although it was worse in the right eye. At that time, he was diagnosed with allergic conjunctivitis and was given an oral antihistamine and topical erythromycin ointment. Later, a visit to the ophthalmologist revealed hyphema and a possible iris mass in his right eye. The patient was referred to the Ocular Oncology Service.
He had been diagnosed with SCLC in May 2021 and treated with radiotherapy and carboplatin, etoposide, and atezolizumab. He was a former cigarette smoker and had discontinued smoking 10 years earlier.
At the initial examination, his BCVA was 20/70 OD and 20/40 OS. IOP was 23 mm Hg OD and 17 mm Hg OS. The anterior segment of the right eye revealed moderate conjunctival and scleral injection with 20% hyphema overlying a milky-white, fluffy-appearing solid vascularized mass involving 6 clock hours of the iris and angle inferiorly (Figure 1). Anterior segment OCT documented the mass in the angle with endothelial touch (Figure 2).
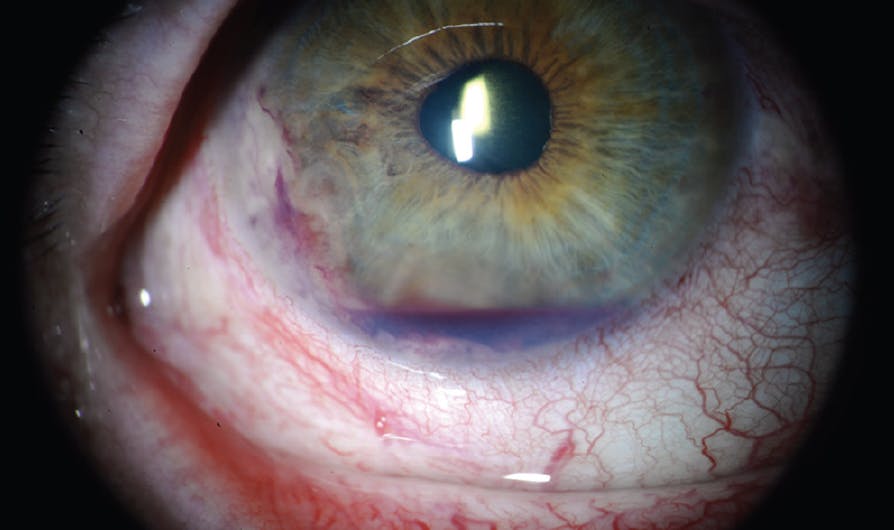
Figure 1. Slit-lamp examination of the right eye documented hyphema, corectopia, and a solid vascularized mass in the inferotemporal angle.

Figure 2. On anterior segment OCT, the transverse cross-section of the right eye showed the tumor at the anterior chamber angle adherent to the corneal endothelium.
On ultrasonography, the mass extended into the ciliary body and the choroid, measuring 24 mm in basal diameter and 6.2 mm in thickness (Figures 3 and 4). The left eye was unremarkable. Given the solid iridociliary tumor and systemic evidence of metastasis, the patient was suspected to have iridociliary metastasis from SCLC. Confirmation via fine needle aspiration biopsy was discussed with the patient, but given the poor systemic status, biopsy was ultimately avoided in favor of treating him directly with external beam radiation therapy (EBRT) to the eye.


Figure 4. B-scan ultrasonography of the right eye showed posterior extension of the mass into the choroidal region.
INCIDENCE AND CLINICIAL PRESENTATION
Of 3,680 cases of iris tumors, solid nonmelanocytic lesions accounted for only 11% of cases, with 2% of all iris tumors representing metastases.6 Most patients with uveal metastasis complain of blurred or decreased vision, while some present with uveitis, episcleritis, or glaucoma-like symptoms due to iris neovascularization or trabecular meshwork blockage.7
In a retrospective review of 104 patients with iris metastasis from systemic cancers, the most common symptoms were corectopia (37%), pain (32%), blurred vision (30%), and secondary glaucoma (30%).8 In 78% of these patients, the metastasis was unifocal and unilateral, as in our case.8 While clinical presentation of both iris melanoma and metastasis can be similar, the diagnosis of iris metastasis is primarily reliant on a history of cancer and evidence of systemic involvement.7,8 However, the definitive diagnosis often requires fine needle aspiration biopsy.7,8
MANAGEMENT OF UVEAL METASTASES
Treatment for patients with iridociliary metastasis from SCLC is generally limited to palliative care. The presence of uveal metastasis frequently indicates widespread systemic disease, as in our patient with brain, bone, and liver metastases.9 One sample of patients with choroidal metastases found synchronous brain metastases in 13% of patients (24 of 188), with an additional 14% (26 of 188) later developing cerebral metastases.9
Our Approach
Systemic chemotherapy and immunotherapy were discontinued in our patient due to idiopathic thrombocytopenia, but he continued to receive palliative radiotherapy for his primary lung cancer. Options to treat his iridociliary metastasis included EBRT, iodine-125 plaque radiotherapy, or enucleation.10 Due to the size and extent of the tumor and his numerous systemic conditions, plaque radiotherapy was avoided, considering the need for surgery and risk of complications with this large tumor.7,11,12 Palliative treatment with EBRT was performed with the aim of preserving vision and preventing intractable pain that could require enucleation.
Benefits of EBRT
There is considerable data on outcomes of EBRT for choroidal metastases, with globe preservation rates as high as 98%.9 One study involving 27 patients with choroidal metastasis from lung cancer treated with EBRT showed 20 (74%) patients who experienced complete regression, three (12%) whose tumor was stabilized, and four (15%) who experienced further growth.11
In another study of 155 eyes with choroidal metastases of various origins, 89 (57%) experienced improved vision or maintained navigational vision (20/60 to 20/200) following EBRT. Among 47 participants who were legally blind (ie, VA worse than 20/400) before EBRT, 17 (36%) experienced improvement to a VA of 20/50 or better or achieved navigational vision.9 Factors associated with a positive response to EBRT included initial VA < 20/50, age < 55 years, White race, and tumor basal diameter < 15 mm.9 One or more radiation-related complications were noted in 28 eyes (12%) and these included radiation retinopathy, optic neuropathy, cataract, neovascularization, exposure keratopathy, and narrow angle glaucoma.9
An additional study focused on the rates and associated factors of complications with EBRT for patients with choroidal and ciliary body metastases.13 Biopsy at the time of diagnosis increased the likelihood of developing complications.13 There was no difference in cataract formation rates between a lens-sparing technique and whole-globe irradiation.13 The median survival time of patients with complications was significantly longer than those who did not experience any complications (25.9 months vs 7.4 months, P = .002), reflecting the relatively late onset of complications.13 In patients with choroidal/ciliary body metastases, these consequences were less likely to occur due to their preexisting unfavorable prognosis.13
CONTROL SYMPTOMS WITH MINIMAL SIDE EFFECTS
While outcomes for iris and iridociliary metastasis were comparatively limited due to less frequent occurrence, EBRT remains a valuable therapeutic option for effectively controlling symptoms of uveal metastases with minimal treatment-associated complications.13
Support provided in part by the Eye Tumor Research Foundation, Philadelphia, PA (CLS). The funders had no role in the design and conduct of the study, in the collection, analysis and interpretation of the data, and in the preparation, review or approval of the manuscript. Carol L. Shields, MD, has had full access to all the data in the study and takes responsibility for the integrity of the data.
1. Cancer facts & figures 2021. American Cancer Society. Accessed May 26, 2023. www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2021.html
2. Basumallik N, Agarwal M. Small Cell Lung Cancer. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
3. Qu Z, Liu J, Zhu L, Zhou Q. A comprehensive understanding of choroidal metastasis from lung cancer. Onco Targets Ther. 2021;14:4451-4465.
4. Shields CL, Welch RJ, Malik K, et al. Uveal metastasis: clinical features and survival outcome of 2214 tumors in 1111 patients based on primary tumor origin. Middle East Afr J Ophthalmol. 2018;25(2):81-90.
5. Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with uveal metastases. Ophthalmology. 1997;104(8):1265-1276.
6. Shields CL, Shields PW, Manalac J, Jumroendararasame C, Shields JA. Review of cystic and solid tumors of the iris. Oman J Ophthalmol. 2013;6(3):159-164.
7. Cohen VML. Ocular metastases. Eye. 2012;27(2):137-141.
8. Shields CL, Kaliki S, Crabtree GS, et al. Iris metastasis from systemic cancer in 104 patients. Cornea. 2015;34(1):42-48.
9. Rudoler SB, Shields CL, Corn BW, et al. Functional vision is improved in the majority of patients treated with external-beam radiotherapy for choroid metastases: a multivariate analysis of 188 patients. J Clin Oncol. 1997;15(3):1244-1251.
10. Shields JA, Shields CL, Kiratli H, Potter P. Metastatic tumors to the iris in 40 patients. Am J Ophthalmol. 1995;119(4):422-430.
11. Shah SU, Mashayekhi A, Shields CL, et al. Uveal metastasis from lung cancer: clinical features, treatment, and outcome in 194 patients. Ophthalmology. 2014;121(1):352-357.
12. Kamran SC, Collier JM, Lane AM, et al. Outcomes of proton therapy for the treatment of uveal metastases. Int J Radiat Oncol Biol Phys. 2014;90(5):1044-1050.
13. Rudoler SB, Corn BW, Shields CL, et al. External beam irradiation for choroid metastases: identification of factors predisposing to long-term sequelae. Int J Radiat Oncol Biol Phys. 1997;38(2):251-256.






_1784132761.jpg?auto=compress,format&w=75)











