
_1696276947.png)
Patients with a full-thickness macular hole (FTMH) have an anatomical defect in the fovea that leads to a significant reduction in central visual acuity and, subsequently, reduced quality of life. While many FTMHs can be idiopathic, they can also be secondary to vitreoretinal traction, high myopia, proliferative diabetic retinopathy, and inflammation.1 The conventional treatment for a FTMH has been pars plana vitrectomy, internal limiting membrane (ILM) peel, and total gas-fluid exchange with long-lasting gas tamponade. This technique is effective in terms of both closure rate and visual acuity improvement, with a 90% success rate for the closure of an acute FTMH noted in numerous studies.2,3 However, alternative treatments for chronic, large, or recalcitrant FTMHs have been developed due to lower closure rates of these subsets of FTMHs with traditional methods.
ALTERNATIVE APPROACHES
Surgeons have recently explored variations of ILM manipulation, such as inverted ILM flaps, ILM free flaps, and hinged ILM flaps. Inverted ILM flaps involve peeling a portion of the ILM and folding it over the macular hole.4 Several studies have looked at using this technique to improve closure rates for large macular holes.5-7 Free flaps can be used when an ILM peel has previously been performed and entail harvesting an ILM flap from a distal site, placing it over the FTMH, and inserting a gas tamponade.8 A prior study noted a success rate of 86% with an ILM free flap compared with a 91.6% success rate for an inverted ILM flap.9
Several studies suggest the ILM flap technique is a valuable option when treating large FTMHs.9 Dera et al noted a 90.8% closure rate when using an ILM flap and a 59.6% closure rate for a conventional ILM peel in patients with a FTMH > 400 µm.10 Another study found similar closure rates of 95.6% and 78.6% for large FTMHs, respectively.11
Not only have these studies shown positive outcomes for ILM flap closure, but many have also hypothesized that the ILM flap acts as a scaffold for migration and proliferation of Müller cells.12 These cells secrete neurotrophic and growth factors that enhance the survival of retinal neurons.12 However, other studies suggest that an ILM flap for a large FTMH has no obvious advantages over ILM peeling related to anatomical morphology and visual function.13,14
In addition to manipulating the ILM, other techniques have been developed for recalcitrant holes. For example, a macular hole hydrodissection includes a standard ILM peel and a soft-tip cannula to reflux fluid into the FTMH, releasing any retina-to-retinal pigment epithelium adhesion at the hole margin.15 An additional technique to consider is autologous retinal transplantation, which has had good success rates but can be technically challenging.16
OUR STUDY
In our recent study presented at the 2023 American Society of Retina Specialists Meeting, we analyzed an inverted ILM flap technique, which entails peeling an ILM flap 2x3 disc diameters wide temporal to and past the FTMH to relieve all traction, laying the ILM back in place, and inverting the temporally peeled portion over the FTMH with insertion of a gas tamponade (Figures 1 and 2). We compared success rates between large FTMHs to determine if one surgical technique is better than another.

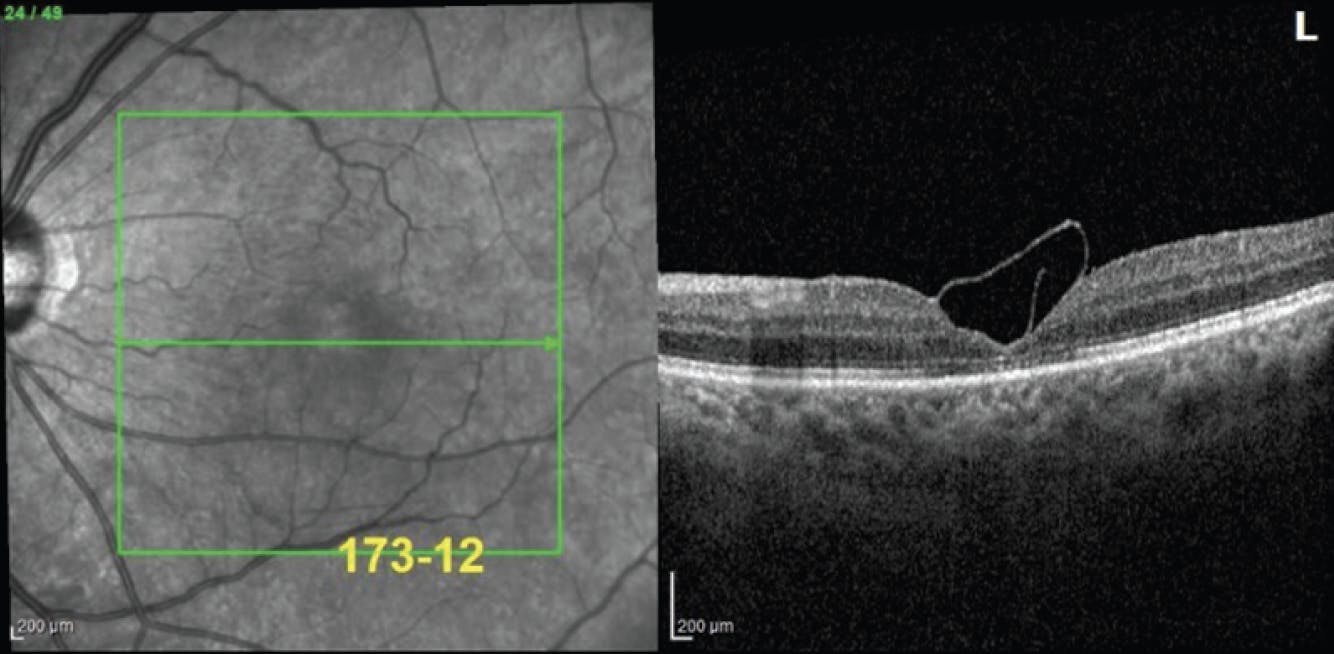
Figure 2. Postoperative OCT showed a closed, chronic FTMH with an inverted ILM flap. Note that the scroll of the ILM overlying the closed hole is visible.
We analyzed available data from a retina-specific practice to compare anatomical and functional outcomes in patients who received surgical intervention for large (> 400 µm) FTMHs by either the ILM flap or peel technique. For overall anatomical outcomes, our study showed an almost identical FTMH closure rate between the ILM flap and peel technique: 94.6% and 93.6%, respectively. Although closure rates were similar within our study, the preoperative mean base diameter was greater in the flap versus non-flap group with a trend toward worse initial visual acuity.
In our subgroup analysis, we looked at FTMH closure rates based on different basal diameters. There was a trend toward lower closure rates for larger holes, which held true for both the ILM flap and peel groups. There was no statistical difference noted between either surgical technique across macular hole diameters. It is unclear if this was due to a limitation in the number of cases studied within each subgroup, the difference in the sizes of the macular holes at onset, or the fact that there is no difference in closure rates between the two techniques.
For overall functional outcomes, there was a statistically significant improvement in both the ILM flap and peel groups postoperatively. These findings are consistent with prior studies overseeing postoperative visual acuity for both treatment groups.17,18 There was an overall improvement in VA of 0.46 logMAR compared with preoperatively in each surgical cohort to the last follow-up. Similar to studies that support visual improvement from 6 months to 2 years postoperatively, our data demonstrated continued improvement within each cohort up to 3 years.19,20
While we have shown that the inverted ILM flap and peel techniques allow for significant anatomical and functional improvement postoperatively, additional research is warranted to distinguish which FTMH scenario responds best to which technique. With many emerging surgical approaches to treat large, complex FTMHs, surgeons must give more consideration to which surgical approach would benefit which patient.
1. Hong-Kee N, Azhany Y, Lieh-Bin O. Full thickness macular hole: early intervention is an important factor in visual prognosis. Malays Fam Physician. 2014;9(3):42-48.
2. Jaycock P, Bunce C, Xing W, et al. Outcomes of macular hole surgery: implications for surgical management and clinical governance. Eye. 2005;19:879-884.
3. Abdul-Kadir MA, Lim LT. Update on surgical management of complex macular holes: a review. Int J Retin Vitr. 2021;7:75.
4. Michalewska Z, Michalewski J, Adelman RA, Nawrocki J. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology. 2010;117(10):2018-2025.
5. Major JC Jr, Lampen SIR, Wykoff CC, et al. The Texas Taco technique for internal limiting membrane flap in large full-thickness macular holes: a short-term pilot study. Retina. 2020;40(3):552-556.
6. Chen G, Tzekov R, Jiang F, et al. Inverted ILM flap technique versus conventional ILM peeling for idiopathic large macular holes: a meta-analysis of randomized controlled trials. PLoS One. 2020;15(7):e0236431.
7. Koçak N, Yeter V, Birinci H. Comparative study of conventional internal limiting membrane peeling versus temporal inverted internal limiting membrane flap for large macular hole treatment. Indian J Ophthalmol. 2023;71(1):188-194.
8. Fung NSK, Mak AKH, Yiu R, et al. Treatment of large, chronic and persistent macular hole with internal limiting membrane transposition and tuck technique. Int J Retin Vitr. 2020;6:3.
9. Velez-Montoya R, Ramirez-Estudillo JA, Sjoholm-Gomez de Liano C, et al. Inverted ILM flap, free ILM flap and conventional ILM peeling for large macular holes. Int J Retina Vitreous. 2018;4:8.
10. Dera AU, Stoll D, Schoeneberger V, et al. Anatomical and functional results after vitrectomy with conventional ILM peeling versus inverted ILM flap technique in large full-thickness macular holes. Int J Retin Vitr. 2023;9:68.
11. Rizzo S, Tartaro R, Barca F, et al. Internal limiting membrane peeling versus inverted flap technique for treatment of full-thickness macular holes: a comparative study in a large series of patients. Retina. 2018;38:S73-S78.
12. Shiode Y, Morizane Y, Matoba R, et al. The role of inverted internal limiting membrane flap in macular hole closure. Invest Ophthalmol Vis Sci. 2017;58(11):4847-4855.
13. Iwasaki M, Kinoshita T, Miyamoto H, Imaizumi H. Influence of inverted internal limiting membrane flap technique on the outer retinal layer structures after a large macular hole surgery. Retina. 2019;39(8):1470-1477.
14. Chen Y, Xu Y, Ye X, et al. The effect comparison of ILM flap and traditional ILM peeling in IMH. Front Med. 2023;10.
15. Felfeli T, Mandelcorn E. Macular hole hydrodissection: surgical technique for the treatment of persistent, chronic, and large macular holes. Retina. 2019;39(4):743-752.
16. Mahmoud T, Moysidis S, Koulisis, et al. Autologous retinal transplantation for primary and refractory macular holes and macular hole retinal detachments: the Global Consortium. Ophthalmology. 2021;128(5):672-685.
17. Kwok AK, Lai TY, Wong VW. Idiopathic macular hole surgery in Chinese patients: a randomised study to compare indocyanine green-assisted internal limiting membrane peeling with no internal limiting membrane peeling. Hong Kong Med J. 2005;11(4):259-266.
18. Nourinia R, Nikzad P, Abolhosseini M, et al. RONA technique: a novel ilm peeling method for treatment of large full-thickness macular holes. Retina. 2023;43(4):692-697.
19. Kwak JJ, Byeon SH. Comparison of long-term visual and anatomical outcomes between internal limiting membrane flap and peeling techniques for macular holes with a propensity score analysis. Eye (Lond). 2023;37(6):1207-1213.
20. Bleidißel N, Friedrich J, Klaas J, et al. Inverted internal limiting membrane flap technique in eyes with large idiopathic full-thickness macular hole: long-term functional and morphological outcomes. Graefes Arch Clin Exp Ophthalmol. 2021;259(7):1759-1771.



_1784132761.jpg?auto=compress,format&w=75)











