


Systemic lupus erythematous (SLE) is a chronic, autoimmune connective tissue disorder affecting multiple organ systems that often follows a clinical course of relapse and remission.1 Retinal disease occurs in 10% to 29% of patients with SLE,2,3 with cotton-wool spots, retinal hemorrhages, and vascular tortuosity being the most common findings.4 SLE retinopathy is usually an indication of severe, active systemic disease and poor prognosis.5,6
Another potential retinal manifestation of SLE is Purtscher-like retinopathy (PLR).6 Purtscher retinopathy (PR) is a rare condition of unknown pathogenesis caused by occlusive microvasculopathy seen in patients with a history of trauma,7 while PLR describes a heterogeneous group of diseases that have similar clinical retinal findings to PR but do not have a traumatic etiology.8 PR/PLR is characterized by the presence of Purtscher flecken, which are seen in half of cases.8,9 Known causes include pancreatitis, renal failure, amniotic fluid embolism, collagen-vascular disorders, and autoimmune diseases.8,10
Here, we report a case of an otherwise healthy patient who presented with PLR, leading to a diagnosis of SLE.
CASE PRESENTATION
A 34-year-old man presented to the hospital with painless vision loss in each eye for 3 weeks, fatigue, body ache, and generalized joint pain. His ophthalmic history included LASIK refractive surgery 1 year prior. On examination, his BCVA was 20/40 OD and 20/25 OS. External eye and anterior segment examinations were normal.
Fundus examination revealed a clear vitreous with multiple peripapillary and perimacular white indistinct polygonal lesions, cotton-wool spots, flame-shaped hemorrhages with venous congestion, sheathing, beading, and cystoid macular edema (CME) in each eye (Figure 1). Mild disc hyperemia was also noted.

Figure 1. Fundus imaging of the right (A) and left (B) eye showed multiple diffuse cotton-wool spots/Purtscher flecken (blue arrow), intraretinal hemorrhage (red arrow), venous congestion, vascular sheathing, and beading that was more prominent in the right eye. CME was also observed in each eye.
OCT of the macula showed CME with a central foveal thickness of 370 μm and 427 μm in the right and left eye, respectively. Fluorescein angiography (FA) showed multiple diffuse arteriolar occlusions and capillary nonperfusion, corresponding to the areas of Purtscher flecken, involving the macula and the peripheral retina with vascular leaking and staining (Figure 2). A diagnosis of bilateral PLR with secondary CME was made. An underlying systemic vasculitis entity was investigated with various laboratory testing, leading to a diagnosis of systemic lupus anticoagulation and antiphospholipid syndrome.
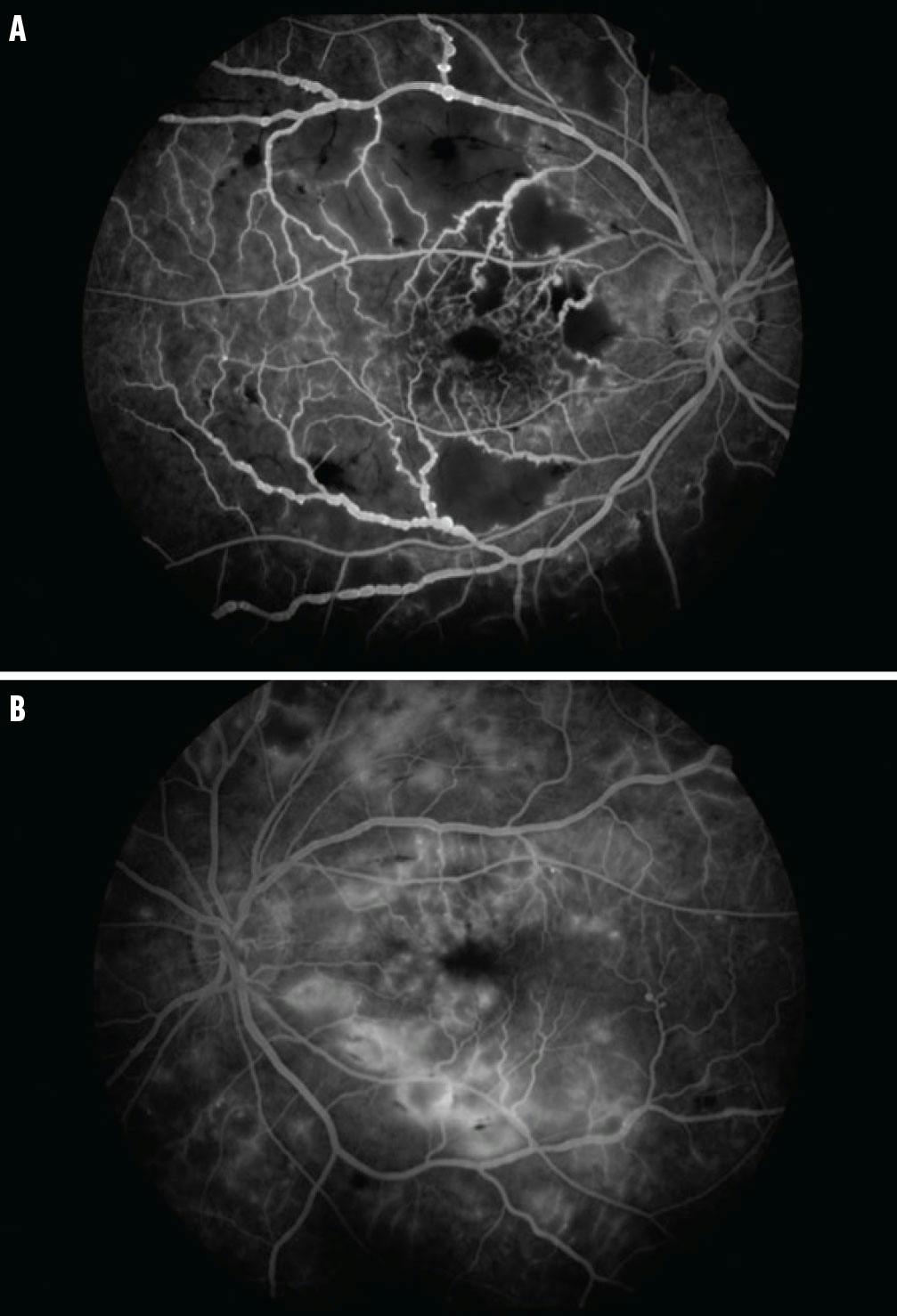
Figure 2. FA of the right (A) and left (B) eye demonstrated diffuse patchy capillary nonperfusion involving the macula and peripheral retina, vessel wall staining, and leakage.
Treatment Approach and Follow-Up
The patient was managed by a multidisciplinary team that included a rheumatologist, neurologist, and hematologist and admitted to the hospital for 1 week for treatment and investigation. He was treated with 1 g/day intravenous methylprednisolone for 5 days with slow tapering over 3 months and was discharged on 1 mg/Kg/day oral prednisolone with a tapering regimen. Two weeks later, he developed deep vein thrombosis and was admitted to the hospital to receive anti-coagulation treatment. The deep vein thrombosis resolved without complication.
The patient was then started on 400 mg oral hydroxychloroquine once daily, 1.5 g mycophenolate mofetil (Cellcept, Genentech/Roche) twice daily, and a 5 mg warfarin tablet once daily, with a plan to continue this treatment regimen for at least 24 months. One month later, OCT of the macula showed residual CME, and an off-label dexamethasone intravitreal implant (Ozurdex, Abbvie) was administered.
His VA had improved to 20/20 OU at this point, and the fundus examination showed the disappearance of Purtscher flecken, cotton-wool spots, and bland intraretinal hemorrhage. OCT confirmed the resolution of CME but showed a wide foveal contour in the right eye with mild atrophic changes in the parafoveal area, indicating ischemic insult. Five months later, he returned with severe blurred vision. Examination showed a hyperemic optic disc and macular edema, and triamcinolone acetonide injectable suspension 40 mg/1 mg (Kenalog-40, Bristol Myers Squibb) was administered in each eye (Figure 3).

Figure 3. Follow-up imaging of the right (A) and left (B) eye revealed the development of a hyperemic optic disc.
Fundus examination 2 months later showed neovascularization at the disc and elsewhere, for which panretinal laser photocoagulation was performed on each eye over multiple sessions. One month later, he developed vitreous hemorrhage in his right eye after an increase in his warfarin dose by his hematologist, and anti-VEGF injection was administered; it was later required to treat vitreous hemorrhage in his left eye as well. Two weeks after resolution of the bilateral vitreous hemorrhage, additional argon laser was performed in each eye. The patient was continued on 5 mg oral prednisolone, hydroxychloroquine, mycophenolate mofetil, and a warfarin tablet.
TIME TO UPDATE THE DIAGNOSTIC CRITERIA FOR SLE?
SLE usually first presents with dermatological symptoms, which include four diagnostic features: malar rash, photosensitivity, discoid lesion, and alopecia.11 The criteria for the diagnosis of SLE includes dermatological and rheumatological signs, renal dysfunction, neurological abnormality, and hematologic and immunologic disorders.14,15 Although retinopathy is seen in 10% to 29% of patients, it is not listed among these criteria.3
SLE retinopathy differs from one patient to another and usually indicates severe, active disease with a poor prognosis.5,7,16,17 Vasculitis of retinal capillaries and local microinfarction are special features of SLE retinopathy. Patients with lupus retinopathy associated with anti-phospholipid syndrome are more prone to develop large retinal vessel occlusion.18,19
Visual prognosis with PLR is variable and depends on the etiology. Pancreatitis, trauma, and male sex are associated with better visual acuity, while patients who are pregnant or have been diagnosed with SLE tend to present with worse visual acuity.7
Our case demonstrates PLR as a first presentation of SLE. A similar case was reported by Alahmadi et al,20 and several retrospective studies and observational case series have shown PLR occurring in patients with SLE.6,7,9,20-23
DIG DEEPER
SLE can have varied ocular and systemic manifestations. Although PLR is not part of the diagnostic criteria for SLE, it can be the first presentation in a patient without dermatological features or systemic disease.
1. Tikly M, Navarra SV. Lupus in the developing world is it any different? Best Pract Res Clin Rheumatol. 2008;22(4):643-655.
2. Read RW. Clinical mini-review: systemic lupus erythematosus and the eye. Ocul Immunol Inflamm. 2004;12(2):87-99.
3. Sivaraj RR, Durrani OM, Denniston AK, Murray PI, Gordon C. Ocular manifestations of systemic lupus erythematosus. Rheumatology (Oxford). 2007;46(12):1757-1762.
4. Ushiyama O, Ushiyama K, Koarada S. Retinal disease in patients with systemic lupus erythematosus. Ann Rheum Dis. 2000;59(9):705-708.
5. Seth G, Chengappa KG, Misra DP, et al. Lupus retinopathy: a marker of active systemic lupus erythematosus. Rheumatol Int. 2018;38(8):1495-1501.
6. Meng L, Yu Q, Zhao X, et al. Purtscher-like retinopathy in systemic lupus erythematosus: clinical features, risk factors and prognosis. QJM. 2023;116(11):923-932.
7. Miguel AI, Henriques F, Azevedo LF, Loureiro AJ, Maberley DA. Systematic review of Purtschers and Purtscher-like retinopathies. Eye (Lond). 2013;27(1):1-13
8. Gil P, Pires J, Costa E, Matos R, Cardoso MS, Mariano M. Purtscher retinopathy: to treat or not to treat? Eur J Ophthalmol. 2015;25(6):e112-115.
9. Agrawal A, McKibbin MA. Purtscher and Purtscher-like retinopathies: a review. Surv Ophthalmol. 2006;51(2):129-136.
10. Massa R, Vale C, Macedo M, et al. Purtscher-like retinopathy. Case Rep Ophthalmol Med. 2015;2015:421329.
11. D’Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet. 2007;369(9561):587-596.
12. Yazdany J, Dall’Era M. Definition classification of lupus and lupus-related disorders. In: Dubois’ Lupus Erythematosus and Related syndromes. 9th ed. 2019;15-22.
13. Doria A, Biasinutto C, Ghirardello A, et al. Photosensitivity in systemic lupus erythematosus: laboratory testing of ARA/ACR definition. Lupus. 1996;5(2):263-268.
14. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725.
15. Petri M, Orbai AM, Alarcon GS, et al. Derivation and validation of systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012;2677-2686.
16. Arevalo JF, Lowder CY, Muci-Mendoza R. Ocular manifestations of systemic lupus erythematosus. Curr Opin Ophthalmol. 2002;13(6):404-410.
17. Kharel Sitaula R, Shah DN, Singh D. Role of lupus retinopathy in systemic lupus erythematosus. J Ophthalmic Inflamm Infect. 2016;6(1):15.
18. Anaya JM, Talal N. Head and neck findings in SLE: Sjögren’s syndrome and the eye, ear, and larynx. In: Wallace DJ, Hahn BH, ed. Dubois’ Lupus Erythematosus. 5th ed. Baltimore: Williams and Wilkins; 1997;783‑791.
19. Ushiyama O, Ushiyama K, Koarada S, Tada Y, Suzuki N, Ohta A, Oono S, Nagasawa K. Retinal disease in patients with systemic lupus erythematosus. Ann Rheum Dis. 2000;59(9):705-708.
20. Alahmadi RM, Hashim RT, Almogairin SM, Abu AM. Purtscher-like retinopathy as a first presentation of systematic lupus erythematosus. Ann Saudi Med. 2016;36(1):85-88.
21. Kunavisarut P, Pathanapitoon K, Rothova A. Purtscher-like retinopathy associated with systemic lupus erythematosus. Ocul Immunol and Inflamm. 2016;24(1):60-68.
22. Wu C, Dai R, Dong F, Wang Q. Purtscher-like retinopathy in systemic lupus erythematosus. Am J Ophthalmol. 2014;158(6):1335-1341.
23. Sellami D, Ben Zina Z, Jelliti B, Abid D, Feki J, Chaabouni M. Purtscher-like retinopathy in systemic lupus erythematosus. Two cases. J Fr Ophthalmol. 2002;25(1):52-55.




_1784132761.jpg?auto=compress,format&w=75)











