

Pediatric rhegmatogenous retinal detachment (RRD) cases are usually managed with a scleral buckle (SB) procedure that involves a 360° limbal peritomy. Although this technique has been the standard for years, it is invasive and requires significant manipulation of the conjunctiva and considerable dissection of the intermuscular septum and other tissues.1,2 Yepez et al introduced modifications to the traditional surgical technique in adult patients, eliminating the need for peritomy.3 While the primary objective is to achieve retinal reattachment, it is equally important to maintain the integrity of the conjunctiva. Here, we detail how we accomplish both in our pediatric patients undergoing an SB.

Figure 1. The transconjunctival grasping technique is illustrated with the inferior rectus muscle. A force duction test is conducted on each muscle to confirm adequate localization.
NEW AND IMPROVED
We recently published our sutureless, peritomy-sparing SB technique for pediatric RRD, ensuring good preservation of the conjunctiva and maximizing recovery of the ocular surface.4 This approach includes the following surgical steps:
Transconjunctival Isolation of Recti Muscles
First, isolate each muscle by grasping it with 0.12 forceps. Next, pass a 2.0 silk suture needle beneath the belly of the muscle and loop the muscle transconjunctivally (Figure 1). Perform a forced duction test to ensure proper isolation. To isolate the superior rectus muscle, make a radial conjunctival incision in the superior nasal quadrant, and use a Jameson hook to avoid the superior oblique muscle.
Treatment of Retinal Breaks
After isolating the recti muscles, visualize the retinal breaks using indirect ophthalmoscopy. Mark the breaks on the conjunctiva and treat them with cryopexy.
Radial Conjunctival Incisions and Scleral Belt Loops
In all four quadrants, make small radial conjunctival incisions several millimeters posterior to the muscle insertion and create scleral belt loops using a crescent blade (Figure 2).
Passing the SB Band
Pass a 41 silicone SB band through the four belt loops and under the four recti muscles. Using a snap or thin, curved forceps helps grasp the band from one radial incision to the other and ensures it is passed fully under the recti muscles (Figure 3). After threading the SB through the belt loops and positioning it under the recti muscles, secure it with a Watzke sleeve in the superior nasal quadrant.
Closure of Radial Incisions
Close the conjunctival incisions with a single absorbable suture or a sutureless technique using a fibrin sealant.

TROUBLESHOOTING
Using anterior segment OCT, researchers reported that children have a significantly thicker anterior conjunctiva compared with adults (280 ± 45 μm vs 239 ± 38 μm), and the difference increases further away from the scleral spur.5 This is due to a higher number of goblet cells and a higher density of conjunctival lymphoid tissue during childhood.6,7 Isolating muscles transconjunctivally in patients with a thick Tenon capsule can be challenging. To overcome this, make radial peritomies near the muscle insertion based on the Spiral of Tillaux. Converting to a conventional SB is always an option.
After vitreoretinal procedures, patients have a higher likelihood of experiencing dry eye disease. This is commonly attributed to the surgical trauma inflicted on the conjunctiva, which in turn results in a reduced density of goblet cells. Studies show that vitreoretinal procedures can decrease the distribution of goblet cells by as much as 40% and the density of goblet cells in up to 60% of cases.8 In a randomized trial in which patients undergoing strabismus surgery were assigned either to a group that received fornix incisions or to a group that received limbal incisions, the latter group had more serious dry eye symptoms and a greater effect on corneal sensitivity and tear film stability.9
Using absorbable braided sutures to close conjunctival incisions can cause ocular surface irritation and hyperemia and increase the tear meniscus height.10,11 A prospective study of strabismus patients undergoing conjunctival closure with fibrin sealant or 8-0 vicryl sutures found that the former group had faster ocular surface rehabilitation.12
Pediatric patients who undergo an SB are at risk of developing glaucoma from the SB or subsequent vitreoretinal procedures.13,14 Studies report that the incidence of glaucoma after an SB can range from 1.4% to 4.4%.15-18 In children, a history of previous ocular surgery can increase the risk of glaucoma surgery failure.19 This may be the result of excessive conjunctival fibroblasts and inflammatory cells.20,21 The limbal peritomy can negatively affect conjunctival health, making it less suitable for glaucoma filtering procedures.
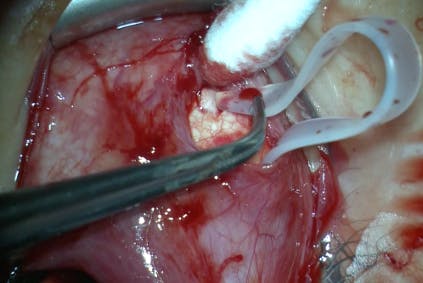
Figure 3. The silicone encircling band is securely threaded through the scleral belt loops and under the recti muscles using radial conjunctival incisions.
A LITTLE FORETHOUGHT GOES A LONG WAY
It is vital to preserve the conjunctiva of pediatric patients for their long-term ocular health. Although doing so can make RRD surgical repair longer and a little more tedious, we believe the time spent is well worth it. Further data and experience with the technique presented here will help refine the approach to SB surgery in children.
1. Nuzzi R, Lavia C, Spinetta R. Paediatric retinal detachment: a review. Int J Ophthalmol. 2017;10(10):1592-1603.
2. Starr MR, Boucher N, Sharma C, et al. The state of pediatric retinal detachment surgery in the United States: a nationwide aggregated health record analysis. Retina. 2023;43(5):717-722.
3. Yepez JB, Murati FA, Petitto M, De Yepez J, Mura M, Kozak I. Peritomy-sparing scleral buckle. Am J Ophthalmol Case Rep. 2019;15:100474.
4. Demian S, Cruz-Pimentel M, Muni RH. Sutureless peritomy sparing scleral buckle in pediatric patients. Am J Ophthalmol. 2024;268:e5-e6.
5. Read SA, Alonso-Caneiro D, Vincent SJ, et al. Anterior eye tissue morphology: scleral and conjunctival thickness in children and young adults. Scientific Reports. 2016;6(1):33796.
6. Kessing SV. Mucous gland system of the conjunctiva. A quantitative normal anatomical study. Acta Ophthalmol (Copenh). 1968:Suppl 95:1+.
7. Österlind G. An investigation into the presence of lymphatic tissue in the human conjunctiva and its biological and clinical importance. H. Ohlssons Boktryckeri; 1944.
8. Mani R, Shobha PS, Thilagavathi S, et al. Altered mucins and aquaporins indicate dry eye outcome in patients undergoing vitreo-retinal surgery. PLoS One. 2020;15(5):e0233517.
9. Li Q, Fu T, Yang J, Wang QL, Li ZE. Ocular surface changes after strabismus surgery with different incisions. Graefes Arch Clin Exp Ophthalmol. 2015;253(3):431-438.
10. Venkatesh R, Jayadev C, Mangla R, Chitturi SP, Mohan S, Ratra D. Ocular surface changes following vitreoretinal procedures. Indian J Ophthalmol. 2023;71(4):1123-1126.
11. Sato T, Koh S, Yasukura Y-i, et al. Surgical factors affecting changes in ocular surface dynamics in the early postoperative period after 25-gauge vitrectomy. Eye Contact Lens. 2019;45(4):254-259.
12. Anand K, Goyal G, Goel Y, Bansal Y, Rastogi A, Jaisingh K. Ocular surface response to fibrin sealant versus vicryl suture for conjunctival closure after strabismus surgery: an objective assessment. Saudi J Ophthalmol. 2020;34(4):243-246.
13. Pinninti U, Carvounis PE, McPherson AR. Scleral buckle surgery and the development of glaucoma - long term follow up. Invest Ophthalmol Vis Sci. 2011;52(14):6154-6154.
14. Kornmann HL, Gedde SJ. Glaucoma management after vitreoretinal surgeries. Curr Opin Ophthalmol. 2016;27(2):125-131.
15. Sebestyen JG, Schepens CL, Rosenthal ML. Retinal detachment and glaucoma. I. Tonometric and gonioscopic study of 160 cases. Arch Ophthalmol. 1962;67(6):736-745.
16. Hartley RE, Marsh RJ. Anterior chamber depth changes after retinal detachment. Br J Ophthalmol. 1973;57(8):546-550.
17. Kreiger AE, Hodgkinson BJ, Frederick AR Jr, Smith TR. The results of retinal detachment surgery. Analysis of 268 operations with a broad scleral buckle. Arch Ophthalmol. 1971;86(4):385-394.
18. Perez RN, Phelps CD, Burton TC. Angel-closure glaucoma following scleral buckling operations. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1976;81(2):247-252.
19. Miller MH, Rice NS. Trabeculectomy combined with beta irradiation for congenital glaucoma. Br J Ophthalmol. 1991;75(10):584-590.
20. Broadway DC, Grierson I, Hitchings RA. Local effects of previous conjunctival incisional surgery and the subsequent outcome of filtration surgery. Am J Ophthalmol. 1998;125(6):805-818.
21. Broadway DC, Chang LP. Trabeculectomy, risk factors for failure and the preoperative state of the conjunctiva. J Glaucoma. 2001;10(3):237-249.


_1784132761.jpg?auto=compress,format&w=75)











