


Central serous chorioretinopathy (CSCR) is characterized by decompensation of the retinal pigment epithelium (RPE) and alterations of the choroidal vasculature, leading to the accumulation of fluid under the macula and, ultimately, serous detachment of the macula.1 The exact mechanism of CSCR involves increased hydrostatic pressure in the choroid and reduced efficacy of the RPE pump.
Increased endogenous cortisol production caused by factors such as psychological stress, depression, and pregnancy can predispose patients to CSCR.2 Additionally, type A personality traits and exogenous corticosteroid use have demonstrated strong associations with the pathogenesis of CSCR due to catecholamine-induced alterations in choroidal blood flow and permeability.3 Research has also identified genetic predispositions and systemic risk factors of CSCR.4
While some cases of CSCR resolve spontaneously, others are nonresolving and require treatment. Such chronic cases, if left untreated, can lead to severe visual decline and even permanent loss of vision.4 Because of the condition’s variable prognosis and complex etiology, CSCR management presents a significant challenge. Current treatment options include laser photocoagulation, photodynamic therapy (PDT), anti-VEGF therapy, and eplerenone; however, concerns have been raised regarding cost, safety, and availability of these therapeutic modalities.5 Subthreshold laser therapy, which uses micropulses to stimulate the RPE without visible retinal damage, offers a potentially safer alternative with quick visual recovery.6 Here, we discuss two cases of CSCR treated with 577 nm subthreshold laser therapy using the TruScan Pro Laser 577 (LIGHTMED) and compare this approach with traditional treatment options.
CASE PRESENTATIONS
Patient No. 1
A 43-year-old woman presented with a diagnosis of CSCR in her right eye and a VA of 20/60 OD. Fluorescein angiography (FA) revealed an expansile dot consistent with CSCR, indicating leakage in the macular area (Figure 1). Given the localization of the leakage and the patient’s visual acuity, the decision was made to proceed with subthreshold laser therapy using a 577 nm wavelength. The patient exhibited significant improvement in VA to 20/30+2 OD 1 month after treatment. She experienced no adverse events, and the fundus autofluorescence performed post-treatment demonstrated no signs of damage (Figure 2).
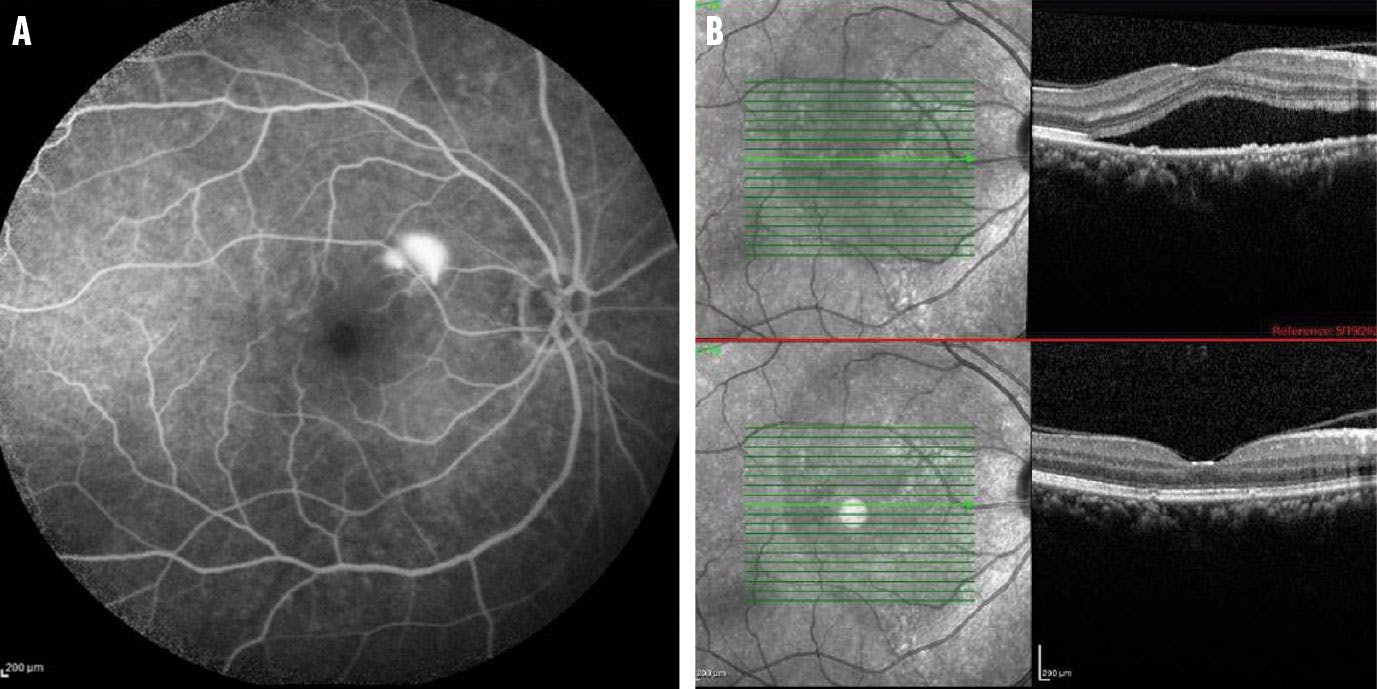
Figure 1. FA of the first patient’s right eye demonstrated an expansile dot consistent with CSCR (A). Comparative spectral-domain OCT imaging revealed a serous retinal detachment in her right eye (B).

Figure 2. One month post-subthreshold laser treatment, the fundus autofluorescence showed resolution of her retinal detachment and revealed no retinal damage.
Patient No. 2
A 55-year-old man sought evaluation for blurry vision in his left eye and presented with a VA of 20/50 OS. FA and ICG angiography demonstrated an expansile dot along the superior arcade with inferior guttering toward the central macula, indicative of CSCR (Figure 3). The decision was made to employ both focal laser therapy at the superior leaking spot, due to its off-center location, and a single session of subthreshold laser within the macula. One month after treatment, a slight improvement in his VA to 20/50+2 OS was noted. This early indication of a positive response to treatment suggested the focal laser successfully targeted the leakage point, while the subthreshold laser stimulated the processes of stabilizing the RPE and reducing subretinal fluid.
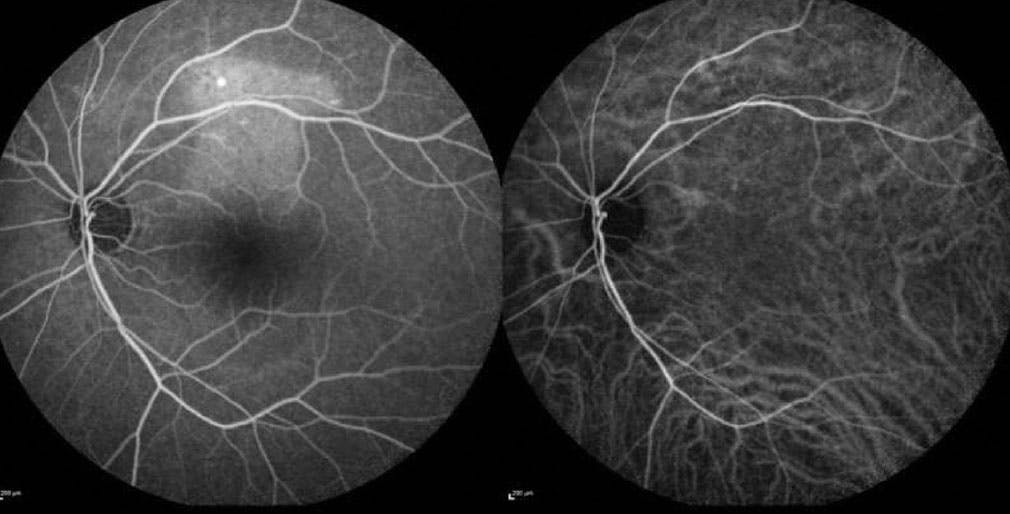
Figure 3. FA (left) and ICG angiography (right) performed for the second patient demonstrated an expansile dot along the superior arcade with inferior guttering toward the central macula, consistent with CSCR.
After 2 months, the patient’s VA showed a pronounced improvement to 20/30 OS with ongoing resolution of subretinal fluid and restoration of the macular architecture; after 6 months, the patient’s VA improved to 20/25-1 OS (Figure 4). This improvement suggests subthreshold laser therapy not only addressed the immediate leakage causing the CSCR, but also promoted longterm retinal health and stability without causing additional damage.

Figure 4. Spectral-domain OCT images of this patient showed evident subretinal fluid in his left eye (A). Six months post-treatment, there was a remarkable improvement in retinal architecture and resolution of fluid (B).
COMPARISON WITH TRADITIONAL APPROACHES
Conventional laser photocoagulation, while a proven therapy in the management of CSCR cases exhibiting clear extrafoveal leakage, works by accelerating the resolution of subretinal fluid and sealing the leakage points; however, this process inflicts irreversible tissue damage and is associated with complications such as scotoma, choroidal neovascularization, and enlargement of the burn-treated area over time.7 Use of 577 nm subthreshold laser therapy would avoid these potential adverse events.
PDT is another established treatment modality, specifically in CSCR cases with subfoveal or juxtafoveal leakage, multiple leaks, or chronic, diffuse RPE decompensation. PDT facilitates choroidal vascular remodeling and induces choroidal hypoperfusion. This approach involves initial intravenous administration of verteporfin, which accumulates in the ocular tissue and is activated by laser irradiation at the leakage points, thereby sealing the RPE defects and potentially mitigating the risk of recurrence in certain cases.8 While the efficacy and reliable safety profile of PDT cannot be overstated, the unavailability of PDT in most outpatient retina clinics, especially in underserved areas, limits its practicality as a therapeutic option.
Eplerenone, a selective aldosterone-receptor antagonist and potassium-sparing diuretic, has also emerged as an alternative therapeutic strategy for CSCR. It is administered orally and, therefore, offers a noninvasive treatment pathway. However, current literature highlights limitations in its effectiveness mainly for certain chronic cases of CSCR.9
Subthreshold yellow laser therapy distinguishes itself by its mechanism of gently heating the RPE without surpassing the threshold for protein denaturation. Its mechanism of action employs a train of short, repetitive pulses ranging from 0.1 to 0.5 seconds, with a brief period between successive micropulses. The time between pulses allows for heat dissipation, limiting the side effects of traditional photocoagulation and targeting the RPE specifically. Practical observations have shown that when a short pulse duration is applied to the retina, only the RPE is affected, with no harm to the inner retinal layers.10 Thus, this innovative approach minimizes collateral tissue damage, a notable disadvantage of laser photocoagulation, by preventing the transfer of excessive thermal energy to the neurosensory retina and avoiding visible burns. Subthreshold yellow laser also is thought to enhance RPE function through the induction of heat shock proteins.11
A WORTHWHILE ADDITION TO YOUR ARMAMENTARIUM
The 577 nm subthreshold laser therapy is a viable option for treating cases of CSCR recalcitrant to standard laser photocoagulation therapy. It can also be done in most outpatient retina clinics, which typically lack the resources and equipment to perform PDT. Large-scale studies should focus on expanding the use of the 577 nm subthreshold laser in the management of CSCR; specifically, there is a need for clinical trials to directly compare its safety and efficacy with that of laser photocoagulation to firmly establish its position within the spectrum of available treatments for CSCR.12
1. Agarwal A. Diseases causing exudative and hemorrhagic detachment of the choroid, retina and retinal pigment epithelium. In: Gass’ Atlas of Macular Diseases. 5th ed. Edinburgh: Elsevier Saunders; 2012:66-91.
2. Haimovici R, Koh S, Gagnon DR, Lehrfeld T, Wellik S; Central Serous Chorioretinopathy Case-Control Study Group. Risk factors for central serous chorioretinopathy: a case-control study. Ophthalmology. 2004;111(2):244-9.
3. Semeraro F, Morescalchi F, Russo A, et al. Central serous chorioretinopathy: pathogenesis and management. Clin Ophthalmol. 2019;13:2341-2352.
4. Liew G, Quin G, Gillies M, Fraser-Bell S. Central serous chorioretinopathy: a review of epidemiology and pathophysiology. Clin Exp Ophthalmol. 2013;41(2):201-214.
5. Goldhagen BE, Goldhardt R. Diagnosed a patient with central serous chorioretinopathy? now what?: management of central serous chorioretinopathy. Curr Ophthalmol Rep. 2017;5(2):141-148.
6. Behnia M, Khabazkhoob M, Aliakbari S, Abadi AE, Hashemi H, Pourvahidi P. Improvement in visual acuity and contrast sensitivity in patients with central serous chorioretinopathy after macular subthreshold laser therapy. Retina. 2013;33(2):324-328.
7. Yannuzzi LA, Slakter JS, Gross NE, et al. Indocyanine green angiography-guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: a pilot study. Retina. 2003;23(3):288-298.
8. van Rijssen TJ, van Dijk EHC, Yzer S, et al. Central serous chorioretinopathy: Towards an evidence-based treatment guideline. Prog Retin Eye Res. 2019;73:100770.
9. Fusi-Rubiano W, Saedon H, Patel V, Yang YC. Oral medications for central serous chorioretinopathy: a literature review. Eye (Lond). 2020;34(5):809-824.
10. Battaglia Parodi M, Arrigo A, Iacono P, Falcomatà B, Bandello F. Central serous chorioretinopathy: treatment with laser. Pharmaceuticals (Basel). 2020;2;13(11):359.
11. Lavinsky D, Wang J, Huie P, et al. Nondamaging retinal laser therapy: rationale and applications to the macula. Invest Ophthalmol Vis Sci. 2016;57(6):2488-2500.
12. Van Dijk EHC, Fauser S, Breukink MB, et al. Half-dose photodynamic therapy versus high-density subthreshold micropulse laser treatment in patients with chronic central serous chorioretinopathy: the PLACE trial. Ophthalmology. 2018;125(10):154711555.








_1784132761.jpg?auto=compress,format&w=75)










