



Myopic traction maculopathy (MTM) involves a spectrum of pathological changes to the macula in high myopia and is caused by two main mechanisms: 1) internal traction due to a posterior hyaloid membrane, rigid vasculature of the neurosensory retina, and/or an epiretinal membrane and 2) external outpouching of the thinned posterior scleral wall (ie, posterior staphyloma).1 MTM comprises numerous posterior retinal abnormalities and can manifest in isolation or combined with posterior vitreoschisis, epiretinal membrane, foveoschisis, lamellar macular hole, full-thickness macular hole, and/or posterior retinal detachment.2
Surgical treatment focuses on addressing the causative mechanisms of MTM and takes two main approaches: 1) an internal approach with pars plana vitrectomy to relieve internal traction by removing the vitreous, epiretinal membrane, or internal limiting membrane and 2) an external approach with posterior scleral indentation (macular buckling) to shorten the axial length of the eye and oppose the sclera, choroid, and retinal pigment epithelium posteriorly toward the photoreceptors of the neurosensory retina.3-7 MTM can be observed or treated either with macular buckling, vitrectomy, or a combination of both.
Here, we describe a novel device and implantation technique—wristwatch macular buckling—that has proven successful in our OR.
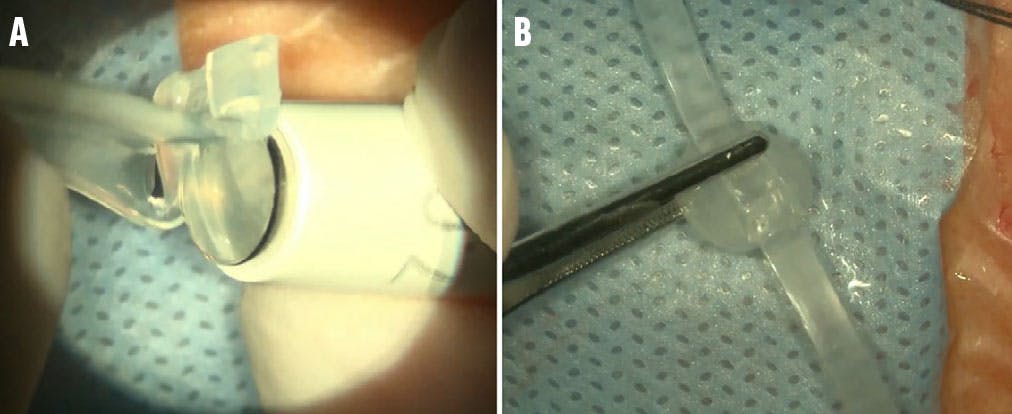
Figure 1. A 7 mm corneal trephine cuts a round indenting head from the silicone (A). The assembled buckling device resembles a wristwatch (B).
THE PROCEDURE
The device, assembled by the operating surgeon prior to implantation, is made of solid silicone rubber that is trephined with a 7 mm corneal punch to harvest a round 7 mm silicone rubber head (Figure 1A). It has a concave internal surface and a preplaced 2.5 mm groove on its external surface made for the silicone band placement.
Use a 2 mm crescent knife to make partial-thickness tunnels at both ends of the external groove, through which the silicone band is passed and firmly fixated. The assembled device resembles a wristwatch, hence its name (Figure 1B).
Perform a circumferential 360° conjunctival peritomy to isolate and sling (using 4-0 silk traction sutures) all recti muscles. Pass the proximal end of the silicone band under the superior oblique and superior rectus muscles and bring it from the superotemporal to the superonasal quadrant. Next, pass the distal end of the silicone band under the lateral rectus and the inferior oblique muscles. Repeat these steps with the inferior rectus. Pull the proximal and distal ends of the silicone band nasally to slide the indenting 7 mm head across the sclera and bring it under the foveal projection.
Confirm the appropriate position of the buckle head through transvitreal observation. Then, use a 2 mm crescent knife to make two partial-thickness scleral tunnels in an oblique fashion in the superonasal and inferonasal quadrants. Pass both ends of the band through the appropriate scleral tunnels and secure them using a Watzke sleeve. Lastly, adjust both ends of the band to center the head of the implant under the fovea while applying mild indentation over the macular region to flatten the posterior staphyloma and reshape the eye wall. Adjust the Watzke sleeves to prevent the band from slipping and help maintain the constant indenting position (Figure 2).

Figure 2. A drawing of the buckling element shows the head indenting the foveal zone and the ends of the band passing through the scleral tunnels, secured with Watzke sleeves.
If vitrectomy and membrane peeling is planned in combination with wristwatch macular buckling, place the buckle implant first and center it properly before conducting the vitrectomy, membrane peeling, and tightening of the buckle to achieve adequate indentation after the vitreous cavity is completely filled with air and prior to the air-gas exchange. Finally, trim the silicone band at both sides, remove the traction sutures from the recti muscles, and ensure Tenon capsule and the conjunctiva are closed.
This buckling method has numerous advantages, including:
- The concave indenting head provides flat indentation, inducing minimal, if any, metamorphopsia.
- Because the indenting head has a large diameter (7 mm), it captures the foveal zone more easily.
- During the procedure, the two-point fixation of the plomb provides flexibility in adjusting both ends of the band and quick centration of the indenting head.
- The procedure doesn’t require lateral muscle resection to access the posterior pole.
- The implant is not related to conjunctival bulging; thus, there is a lesser probability of extrusion.
- The buckle is fixed onto the sclera without sutures.
- The device does not require customized manufacturing and is cost-effective.

Figure 3. This patient’s MTM involves vitreomacular traction (A), an epiretinal membrane (B), foveoschisis, and posterior retinal detachment (C). Seven months post-vitrectomy and supplementary macular buckling, the retina is attached with minimal subretinal and intraretinal fluid (D and E). B-scan echography shows a posterior scleral outpouching and a reshaped staphyloma due to the buckle indentation (F).

Figure 4. This patient has preoperative vitreoschisis, retinoschisis, and a posterior retinal detachment. Postoperative months 1, 3, and 6 show reabsorption of subretinal fluid and reduction of retinoschisis that is directly related to gradual improvement in visual acuity.
CASE STUDIES
At our center, we operated on seven eyes of six MTM patients between April 2023 and November 2024. We performed wristwatch macular buckling with pars plana vitrectomy and membrane peeling in six eyes and macular buckling alone in one eye.
All patients achieved good functional and structural outcomes, including retinal reattachment, macular hole closure, and retinoschisis resolution. Visual acuity improved in all except one patient, in which the retina was reattached and the central scotoma disappeared but BCVA didn’t change from baseline (Figure 3). In the case where standalone macular buckling was performed, intra- and subretinal fluid is still in the process of reabsorption (Figure 4).
Macular buckling is beneficial in certain cases of MTM where retinal tissue is insufficient and unable to cover the broad area of posterior staphyloma, making macular hole closure difficult. Mastering this procedure requires a learning curve to avoid damaging the optic nerve and inducing excessive metamorphopsia related to high buckle indentation.
1. Kumar A, Chawla R, Kumawat D, Pillay G. Insight into high myopia and the macula. Indian J Ophthalmol. 2017;65(2):85-91.
2. Johnson MW. Myopic traction maculopathy: pathogenic mechanisms and surgical treatment. Retina. 2012;32 Suppl 2:S205-S210.
3. Lu L, Li Y, Cai S, Yang J. Vitreous surgery in highly myopic retinal detachment resulting from a macular hole. Clin Exp Ophthalmol. 2002;30(4):261-265.
4. Qu J, Zhao M, Jiang Y, Li X. Vitrectomy outcomes in eyes with high myopic macular hole without retinal detachment. Retina. 2012;32(2):275-280.
5. Kuhn F. Internal limiting membrane removal for macular detachment in highly myopic eyes. Am J Ophthalmol. 2003;135(4):547-549.
6. Alkabes M, Mateo C. Macular buckle technique in myopic tractio maculopathy: a 16-year review of the literature and a comparison with vitreous surgery. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):863-877.
7. Cyrino FVR, de Lucena MM, de Oliveira Audi L, et al. Historical and practical aspects of macular buckle surgery in the treatment of myopic tractional maculopathy: case series and literature review. Int J Retina Vitreous. 2024;10(1):60.










-1_1748961738.jpg?auto=compress,format&w=70)

_1784132761.jpg?auto=compress,format&w=75)











